
Function
-
Posts
926 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Everything posted by Function
-
I think, no. Anyone with active suicidal thoughts is believed to not be of "sound" mind. Suicide often leads from mental illnesses, such as depression, which most of the time can be treated; denying adequate treatment would be wrong. If refractory, or untreatable, leading to unbearable suffering, in some countries, like here in Belgium, one can ask (and run through some procedures) for euthanasia.
-
Accepted for a residency in anaesthesiology!
-
Finally graduated magna cum laude as an MD.
Although I have received the wonderful opportunity to specialise in neurosurgery, being a neurosurgery resident is just a dog's life I could not lead for the lengthy duration it has. Because of lots of reasons, I've decided to carry on as an aspiring future anaesthesiologist.
-
Hi guys For a case presentation in neurosurgery, I'm talking about the Jannetta procedure, in which, in patients with a neurovascular conflict between a cranial nerve and an offending vessel (mostly an artery compressing the nerve and pulsating against it), a sponge-like matter (Teflon, Merocel ...) is surgically inserted between the nerve and the vessel. I'd like to briefly talk about how the sponge absorbs most of the pulsatile energy/impact of the vessel, preventing energetic transmission to the nerve. I can't seem to find, however, a physics model explaining this. Does someone have a good explanation on how sponge-like matters absorb kinetic energy and prevent transmission of most of that energy past itself? Thanks! Function
-

Brain damaga due to psychosis
Function replied to Hans de Vries's topic in Psychiatry and Psychology
During my psychiatry internship, most psychotic delusions (and also delusions in, for instance, major unipolar depressive disorder with psychotic features) were such delusions. The tricky part is identifying whether this delusion or idea can be contradicted to the patient, or not. For instance, we had one female patient in her 40s, with the undeniable idea (ergo, delusion) that she was having Alzheimer's dementia. This made her "normal" major unipolar depressive disorder one with psychotic features, making her immediately eligible for electroconvulsive therapy. The delusion became more of a deniable idea as time progressed. I think this is still a psychotic feature. Not knowing it's not real, that is, acknowledgeing the hallucination as something real, to me, is a delusion. But I'm not sure as to what guidelines and such state about this. -
Brain damaga due to psychosis
Function replied to Hans de Vries's topic in Psychiatry and Psychology
Actually, schizophrenia is one of the "psychosis spectrum disorders", and "psychosis" as such is more of a syndrome, rather than a symptom in itself. A psychosis is an event or episode characterised by either hallucinations, delusions, very chaotic or catatone behaviour, inconsistent speach, or negative symptoms. For schizophrenia, at least two of these "psychotic" characteristics should be present (the "A criterium" for schizophrenia) for a duration of at least 6 months. Comparably, schizophreniform disorder is basically the same, but lasts between 1 month and 6 months. -
Brain damaga due to psychosis
Function replied to Hans de Vries's topic in Psychiatry and Psychology
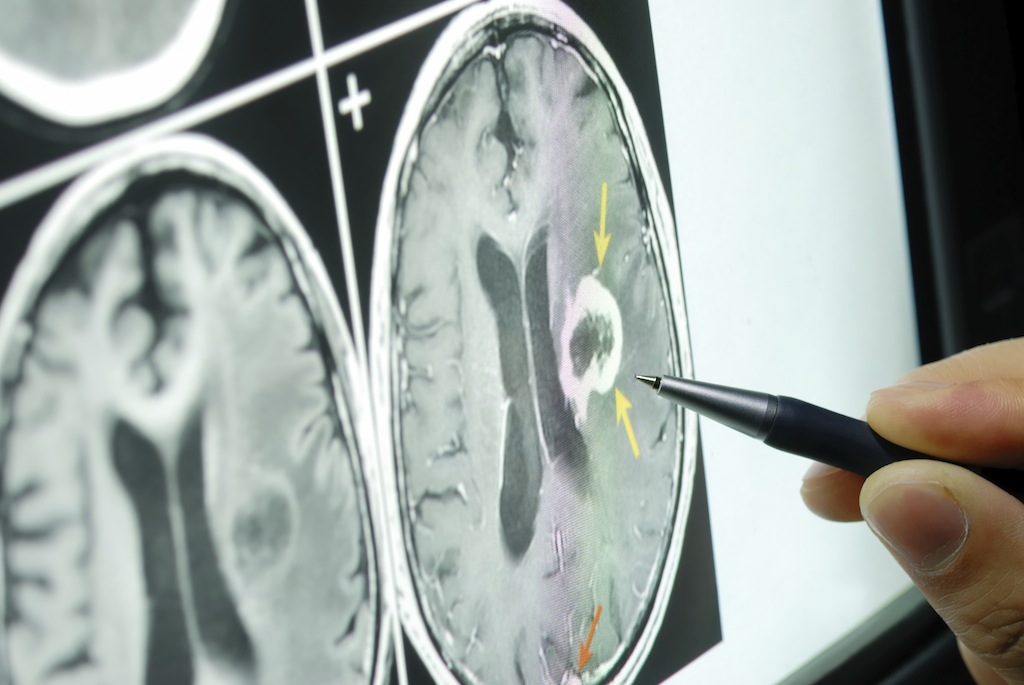
In the tertiary care centre where I had my internship, yes, they did, as should be done quite routinely to exclude large organic causes (such as acquired brain injuries) for their pathology. Here, it's important to not that it's a tertiary care centre we're talking about. As a GP, you shouldn't have MRI scans done of anyone seeing you for depression ... -
Brain damaga due to psychosis
Function replied to Hans de Vries's topic in Psychiatry and Psychology
I do not feel like citing the correct references, but as a matter of fact, yes. Nearly all psychiatric illnesses have organic impact on the brain. And not a good impact, for that matter. During my internship in psychiatry, I observed a lot of MRI scans of people admitted with depression, psychosis, bipolar disorder ... 1 thing they had in common: white matter lesions. -
The importance of publishing as a masters student - or not?
Function replied to limit's topic in Science Education
If you're doing an MD, publishing opens doors to further specialisation. -
The news about that black hole thing made me think. Now forgive me, physicists and others, for being such a noob when it comes to astronomy, but I had this idea, which didn't sound too stupid to me, but again, I'm a real layman in astronomy.
I was thinking that the big bang may have been a black hole, being overloaded with everything else the universe held, such that it became unstable, and exploded? Additionally, if I'm right, black holes grow while eating stuff, and may eat each other. What if our whole universe will come to a point in time where there are only two black holes, which have eaten anything else, remaining only for one to eat the other one, leaving only one giant black hole, once again being overloaded, and exploding, like a new big bang?
-
In the hospital environment, a lot of letters must be written. I'm looking for a way to standardize all letters I'm making. To do so, I would like to make a MS Office Word wizard, which just asks me all relevant things (e.g., salutation, patient name and birth date), lets me select all things in clinical examination that are deviant from a list ..., and then merges everything into a standardized document, which would be a bit easier than making a template.
Does anyone know how I can do this?
-

There is a whole vertical IT industry dealing with adressing what you wrote plus much more. There are specialized genre of software dealing with medical needs alone, those include everything from ticketing, registering a patient, printing stuff, keeping dynamic databases accesable for different pieces of software and a lot more - everything that needs to be done to fulfill any medical environment. Its a competive market where everything that needs to be provided has been provided, I would suggest you look into talking to your hospital IT guy...I know he presumably might not be too hot as IT guys tend to be not too interesting but hey, you gotta deal with it

-

-

-
-
For once, I passed all my exams with great distinction, and my thesis specifically with greatest distinction

Let's hope my internships (starting March until July 2020) can help me finish my Master with great distinction ...
-
Defended my thesis in front of the examination board. They were very pleased, found both the thesis and the presentation excellent, appreciated my direct and to-the-point answers to their questions ... Couldn't ask for more! 8 February is verdict day ...
-
Feel free to watch this:
-
Supervisors were happy with my thesis, said it could easily be a PhD dissertation
 to be defended on 21 January ...
to be defended on 21 January ...
-
First full version of my thesis complete! To be revised by my supervisors, and to be printed

-
is homosexuality unnatural and can be cured?
Function replied to Bucky Barnes's topic in Other Sciences
Missed those allegedly self-conscious flippin' creatures. My bad. -
is homosexuality unnatural and can be cured?
Function replied to Bucky Barnes's topic in Other Sciences
Please, give solid arguments why you think that. Above all, humans and higher primates are thought to be the only species to enjoy sex, and not only do it for reproductive purposes. So imho, this statement becomes false. -
Concerning type 1 errors: each patient had received a MR spectrum. Each spectrum had some characteristics (11, to be precise, of which 1 was categorical, the other ones continuous), which were all subjected to Shapiro-Wilk (in each subgroup per comparison), and variables with allegedly nonnormal value distributions were log-transformed, and the test was run again. And then, all variables were compared each time between 2 distinct groups (e.g., high-grade tumours v. low-grade tumours). I applied a Bonferroni correction in post hoc tests where more than 2 tumour categories were present (e.g., grade I v. grade II v. grade III v. grade IV), or when the categorical variable (which had 3 categories) turned out to be significantly different between any two (or more) groups. Post hoc chi-squared or Fisher's exact tests were then run, with Bonferroni correction applied to the significance level. For the other analyses, there was no need for type 1 error correction, as one could interpret each comparison to be a separate "study". Additionally, no variables were ever combined into one predictive model. That would have led me too far. I'll look for some articles that are representative for in vivo MR studies.
-
There are differences in other parameters within comparisons of other groups, but for this one group–group comparison, only this variable differs significantly. I already implemented everything that’s usually used as parameters in MR spectro in human brains, but thought of ‘designing’ new parameters. Edit: after all, I aimed not only to confirm what is already known, but to develop some more unusual variables, as we are in search for optimisation of noninvasive diagnostic methods in tumour assessment
-
I am looking at the entire spectrum, but certain frequency peaks represent very distinct metabolites. Change in protractor direction, would that actually not be exactly the same as adding 90 degs to every measured angle post hoc? And that’s the stupid part: a nonparametrical comparison of the original angles does not differ significantly between 2 groups, whereas the Briggs log of the angles + 90 degs does. And as my thesis actially focusses on tumour group classifications, I wouldn’t just consider this as a methodology designed “just to find something significant at one point”, but as a methodology to find and describe class predictors. First step in such process is assessing differences in parameter distributions between both groups ...
-
Log and square root transformations are common transformations in statistics for variables that are nonnormally distributed, hoping to achieve normality in their log- or root-transformed variants. Which I got. IBM argues that it is possible to "add a constant big enough" to all values, such that no value is negative or zero, and then apply log transformation. An advantage to this method would be that simply adding a constant to each value does not alter variance amongst variable values. The situations you present are highly unlikely. We're talking about proton NMR spectroscopy of some in vivo metabolites. Achieving the situations you suggest are nearly impossible, as the peaks themselves will just stay where they are, and only chance in amplitude, not in frequency/chemical shift, which is displayed on the horizontal axis.
-
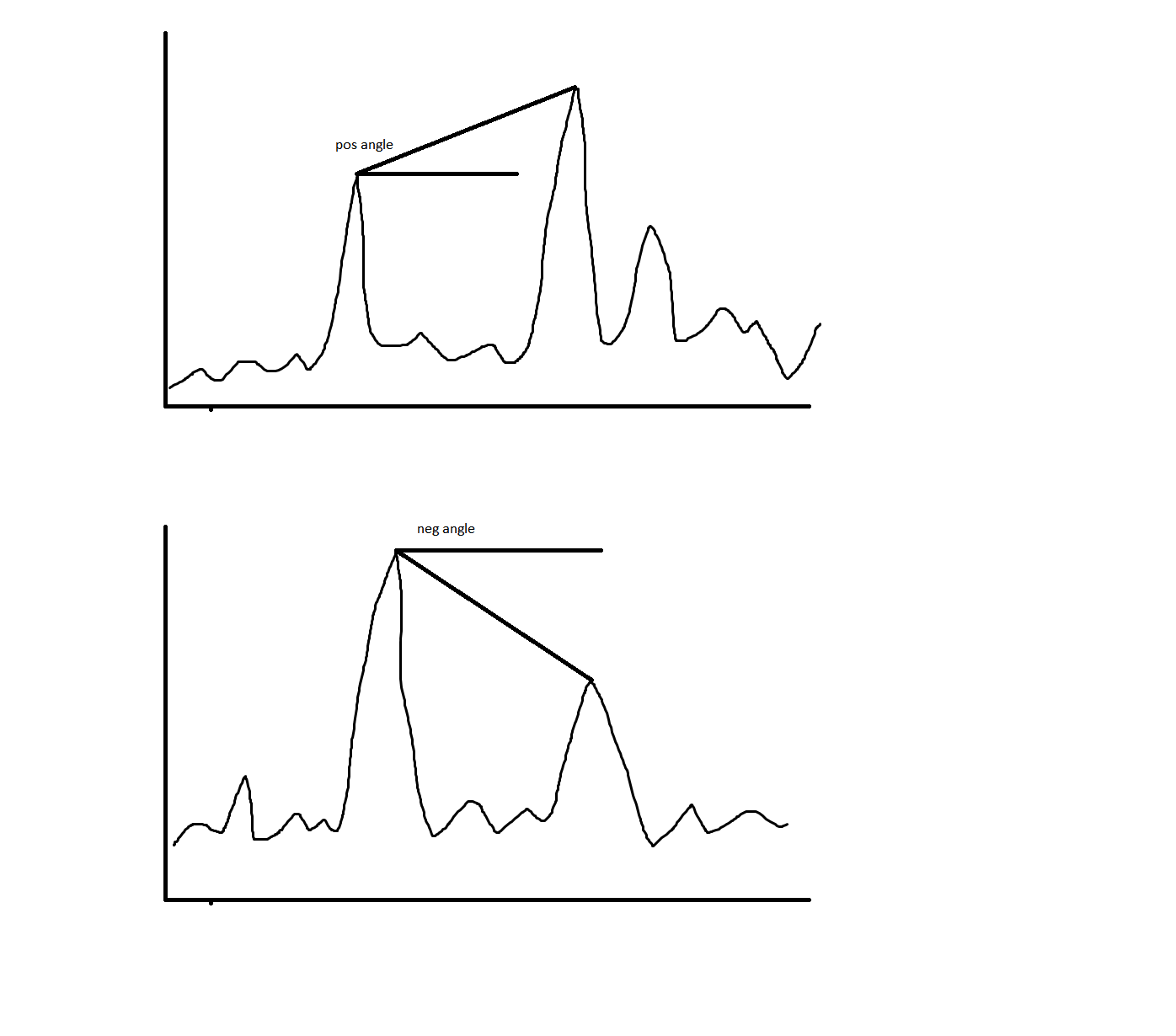
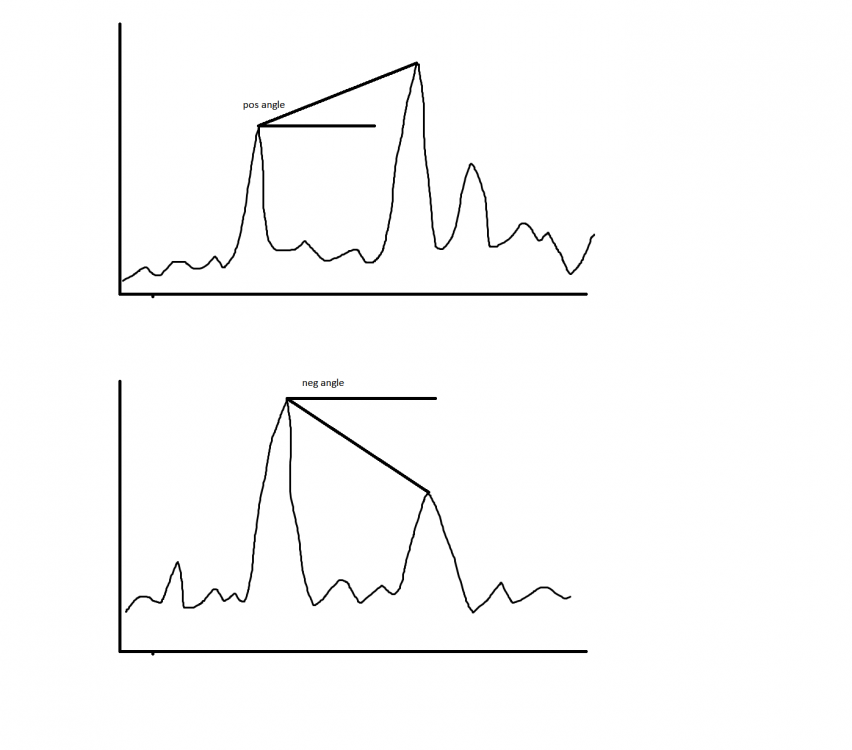
Because that's how I defined my angle. It's always defined as the angle the line (or, if you like, vector) from the first to the second peak makes with a horizontal line. I wouldn't have liked working with (360° - (negative angle value)) to substitute the negative angles, as then I would have to conclude that the second situation would have a larger angle, which, according to the definition I gave to that angle, is absolutely not the case. The sign of the angle is inherently correlated with the characteristic of both peaks relative to one another (first peak higher, or second peak higher). The constant arrangement of both peaks on the horizontal axis made me define the angle to be indisputably either greater than -90°, or smaller than 90°. "Log transform a variable" is performing a natural Briggsian logarithm on all its values, and saving the results as values of a new variable.
-
Hello everyone For my thesis, I'd like to log transform a variable that represents a certain angle between 2 peaks on a curve. The problem, of course, is that this angle can be negative. As no angle is smaller than -90°, would it be allowed to add 90° to all angles, and log transform the results into a new log-transformed variable? Thanks F
-
Hello y'all In my thesis, I have this variable, which is expressed in a percentage (%). It's not an option to, e.g., display 20 % as 0.20, since that is absolutely not common for that variable. Now, this variable does not satisfy the conditions for parametric testing. However, its square-root variant does. But if I report both this variable, in %, then do I have to change the "unit" (which in itself is demensionless) to something else than %? Now I would report: Mean Var ± SD - % Mean VarROOT ± SD - % But I'm not sure if this is quite right. After all: e.g., in the case of 20 %, I took the root of 20, and not of 0.20. So ... sqrt(20 %) = sqrt(20) * sqrt(0.01) = 4.47 * 0.1 = 0.447 ~ 44.7 % And sqrt(0.20) = 0.447 ~ 44.7 % But erm ... Is there a symbol for 1/10? Because now I see that I would incorrectly report 4.47 % (since I only rooted 20 without the %) instead of 44.7 %. Thanks F