Peter Dow
-
Posts
129 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Everything posted by Peter Dow
-
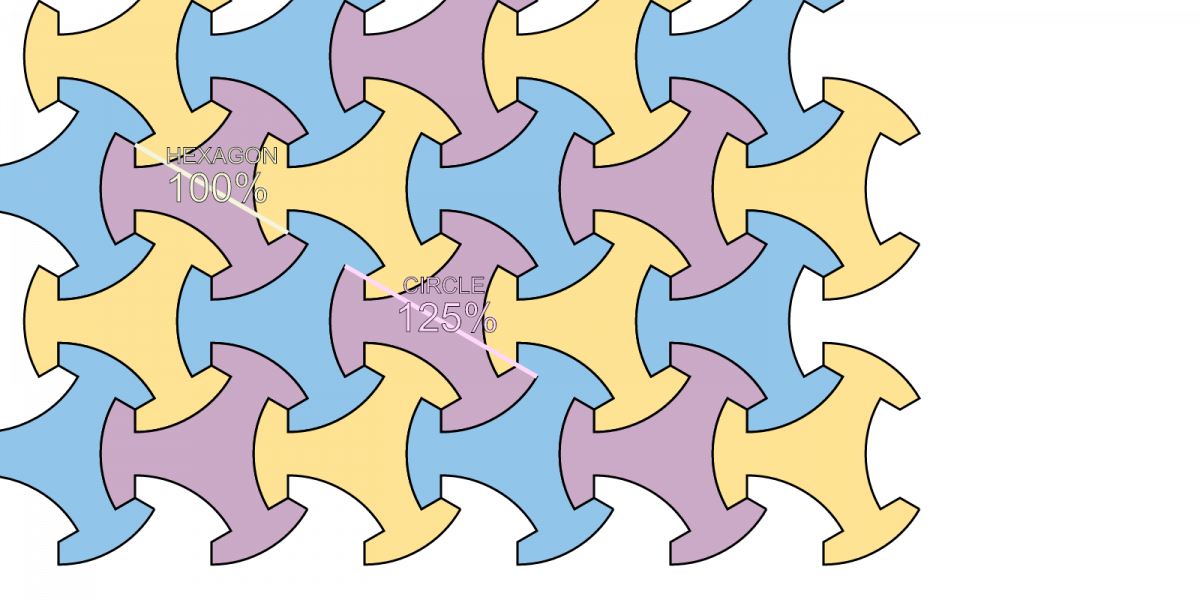
 Trispokedovetiles Animation Webpage I've programmed a webpage using Javascript to display an animation which shows a range of different trispokedovetiles, each of which can be specified by a "CIRCLE" percentage, which is the ratio as a percent of two parameters - 1. A "HEXAGON" parameter length - always nominally "100%" 2. A "CIRCLE" parameter length - the animation varies this between 100% and 135%, though up to 150% is possible in theory. So you can specify the "CIRCLE" percentage to specify a particular shape of trispokedovetile. A still image from the animation is attached - showing trispokedovetiles with "CIRCLE" = 125%. I've tested the animation in Chrome and Internet Explorer browsers and it works fine for me. But it is not working in Firefox for some as yet unknown reason. Let me know by replying here if you have any other problems with the animation not displaying for you.
Trispokedovetiles Animation Webpage I've programmed a webpage using Javascript to display an animation which shows a range of different trispokedovetiles, each of which can be specified by a "CIRCLE" percentage, which is the ratio as a percent of two parameters - 1. A "HEXAGON" parameter length - always nominally "100%" 2. A "CIRCLE" parameter length - the animation varies this between 100% and 135%, though up to 150% is possible in theory. So you can specify the "CIRCLE" percentage to specify a particular shape of trispokedovetile. A still image from the animation is attached - showing trispokedovetiles with "CIRCLE" = 125%. I've tested the animation in Chrome and Internet Explorer browsers and it works fine for me. But it is not working in Firefox for some as yet unknown reason. Let me know by replying here if you have any other problems with the animation not displaying for you.
-
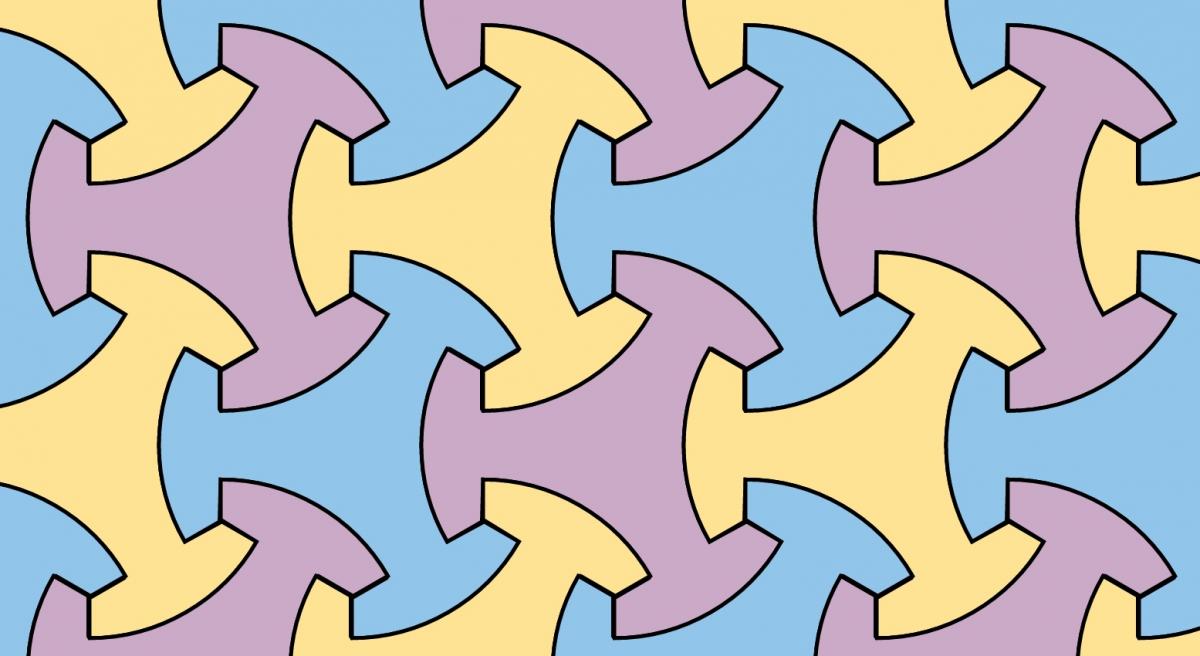
I'm going to try for the "Mathematics" forum for this topic but no worries if the mods decide to move this to "The Lounge". I've posted this image which I've described as a "Three-spoke dovetailing tile tessellation". Trispokedovetile tessellation by Peter Dow, on Flickr which is a tessellation of this tile shape, Trispokedovetile by Peter Dow, on Flickr Check my Flickr page for the preceding design iterations and inspiration. I've named the shape Trispokedovetile which is a contraction of "tri-spoke dovetailing tile". "tri-spoke" because the shape is similar to a 3-spoke motorcycle wheel with three bites taken out of it. "dovetailing" because the tiles interlock like a dovetail joint But it is quite possible this shape is already known to geometry and already has been named. Do you know if this shape has already been named? If so please do reply to tell me what the name is.
-
I'm calm but not complacent. I'm in trouble and I need a good defence. I did apologise. To quote from one of my emails to the prosecutor, court etc. No shit Sherlock. Don't judge a book by its cover. I want a family, to become a father but have had no success with women as a younger man, or screwed up my chances, so now child-bearing age women are that much younger than I am.
-
I'm a Scottish scientist and I'm in big trouble! I'm on trial for my @ peterdow tweets Trial date - Aberdeen Sheriff Court, 4th November 2015 The tweets I posted on my @ peterdow Twitter account in July 2014, two months before the Scottish independence referendum, employed republican political rhetoric to try to express in the strongest possible terms my political support - for a republic to replace the kingdom and for an elected president to replace the monarch as head of state. I link from my @ peterdow Twitter account to my Scottish National Standard Bearer website at SCOT.TK where I dutifully explain the reasons why the people of Scotland would do better, be safer and be more prosperous, if we exercise our political right to establish a Scottish republic. None of my tweets were literal "threats" or literally "threatening" that I or anyone else could, would or should "threaten" the Queen. My tweets were no more "a threat" to the Queen than Alex Salmond's "hold Westminster's feet to the fire" was a "threat" to anyone in Westminster. The police didn't arrest Salmond for making criminal "threats" for the same reason as the police shouldn't have arrested me. Politicians and political authors alike sometimes use rhetorical language. In my tweets I have employed rhetoric such as figures of speech, hyperbole, brevitas and synecdoche and such tweets cannot reasonably be interpreted literally. Peter Dow with his school, college and university degree certificates I'm a scientist with many qualifications and a science degree from Edinburgh University. I am an intelligent and educated man and I know the difference between "intelligence and education" and "stupidity and ignorance". My scientific opinion is that it was stupidity and ignorance on the part of police detectives, prosecutors and sheriffs who read my tweets and quoted them as their poor excuse - to seek a sheriff's warrant to incite police officers to force entry to my home, search it and take my property to break my front door down, as the police did, on 27th July 2014 to arrest me, to charge me and to hold me in a police cell overnight, to ransack my flat from top to bottom, damaging my property in the process, to seize my computer and my memory devices holding my irreplaceable science research and development data to refuse to return my property even when it is not needed as "evidence" to "prove" anything because I admit the @peterdow tweets were mine to impose in Aberdeen Sheriff Court oppressive bail conditions requiring me not to access the website of scot.tk or social media, with the threat that bail would be withdrawn and I would be imprisoned until trial - and that's a real threat of police and prison officer violence against me to terrorize me from posting about my political views on social media, which at that time would have been increasingly about the campaign for the Scottish independence referendum, supporting a "YES" vote to trump up a criminal charge in respect of my social media posts to proceed to a unfair trial in Aberdeen Sheriff Court on 4th of November I frankly and openly admit to owning the @ peterdow Twitter account and I've offered to delete any of the complained-about tweets which the police or prosecutors would otherwise take action over because no tweet is worth the loss of liberty and property which the police and prosecutors have terrorized me with. I would note in passing that gagging YES-campaigners, banning any of us from social media, rigged the indy-ref campaign in favour of a "NO" result. Banning those like me who disagree with the so-called "Edinburgh Agreement" (which, unlike Salmond & Sturgeon, I would not have signed) - rigged the unjust outcome of Scotland still firmly stuck in the UK, ignoring the legitimate demand for a 2-state solution, which would mean establishing an independent Scottish state now, as is the democratic right of the 1.6 million people and the 4 council areas who voted "YES". Although I am not a lawyer, it seems to me that all this unjustified police state violence and threats which I have suffered is in violation of my human rights in law under these articles of the European Convention of Human Rights - Article 5 - liberty and security Article 6 - fair trial Article 8 - privacy Article 9 - conscience and religion Article 10 - expression Article 11 - association Article 13 - effective remedy Article 14 - discrimination All of those ECHR articles, except 13, have been incorporated into UK and Scottish law. So if anyone should be on trial for breaking the law, it is those police and law officers of the state who have violated their duty and violated my legal human rights. I propose that stupid and ignorant police officers and prosecutors should be dismissed from their employment everyone should exercise their viewer discretion whether or not to read the strong language which is to be found on Twitter and police and prosecutors should leave people like me posting harmless posts on social media well alone. Sadly, the reality is that "stupid and ignorant police officers and prosecutors who insist on arresting and prosecuting people for their harmless tweets" is what Scotland is cursed with now thanks to the dreadfully incompetent leadership of - Chief Constable Sir Stephen House and Lord Advocate Frank Mulholland who should both be sacked. Aberdeen is doubly cursed with a dreadfully incompetent area Procurator Fiscal, Andrew Shanks who should also be sacked. I'm innocent of any crime and no miscarriage of justice can accurately paint me as "a common criminal", because I could only ever be a political prisoner - unjustly arrested, unjustly prosecuted and perhaps unjustly convicted and unjustly punished for lawfully expressing my democratic political views. The tyranny of the police, prosecutors and courts in this bad kingdom is one of the reasons I am a republican. I believe that we, the people, would serve ourselves more fairly by electing a president as a helpful head of state, not only a figurehead - someone with a duty to hold the officers of the state to account for their abuses. Save my science Scientists must be allowed to get on with our scientific duties in the public interest and in the service of humanity. I have published new scientific and engineering concepts and proposals regarding - making renewable energy more competitive, efficient and practical mathematics to maximise energy generated from wind turbines 'farms' designs for super-sized hydro-electric pumped-storage schemes an approach towards a cure for cancer a prototype of a cheap cryo-surgical instrument - my 'freezerbaton' H-shaped super-bricks for assembling stronger, lighter structures other published ideas in various scientific fields My irreplaceable science research and development data was held on the computer and memory devices seized by the police. I need that data returned to me urgently to allow me to continue with my scientific duties, as I requested of First Minister Nicola Sturgeon when she appeared with her cabinet secretary colleagues, here in Aberdeen, in February 2015. VIDEO of Peter Dow asking First Minister Sturgeon this question - VIDEO - First Minister Sturgeon replies to Peter Dow Later that evening in February 2015, I spoke to Justice Minister Matheson, as First Minister Sturgeon had suggested and I passed to him a copy of my document explaining the circumstances and demolishing the flimsy case against me and requesting that the charges be dropped and that my computer equipment be returned to me. Mr Matheson agreed to pass on my document to the law officers and I have anyway emailed the law officers directly myself. In all the 8 months since February 2015, the law officers have neither ensured that the Procurator Fiscal Service drop all charges against me nor have the law officers seen to it that the police return my computer equipment and irreplaceable science research data. So I've long since run out of patience with the Scottish government's law officers, who are the failing Lord Advocate Frank Mulholland and the failing Solicitor General Lesley Thomson. My opinion now is that the Scottish government's law officers should be summarily sacked and replaced by the First Minister because these law officers have violated their duty to ensure that the Procurator Fiscal Service should not prosecute citizens for our political viewpoints and should not violate citizens' legal human rights to freedom of expression. These failing law officers cannot be trusted with independence from government, nor from the people's elected representatives. I therefore recommend that these law officers be held accountable for their failings and be summarily dismissed from their offices. A crime against humanity To interrupt my scientific duties and service to humanity with a police raid and court action amounts to the state harming the public interest and committing a crime against humanity. No state and no officer of the state should ever dare to obstruct what even one scientist can do for the prosperity of the people and for the benefit of humanity because there can be no "state immunity" for crimes against humanity, as the Nuremberg Trials demonstrated. No justice for republicans in Queen's courts I have been victimized, traumatised and offended against in this case and in other cases before this one, by what the sadistic and vindictive police, prosecutors, courts and prisons have unjustly and illegally done to me when, as a good man with a keen social conscience, I have bravely tried to do my duty to my neighbours, my community, my home city of Aberdeen and my country of Scotland and suffered arrests and imprisonment for my good deeds. There is a saying "no good deed goes unpunished". Indeed, it does seem to be true anyway that no good deed by a republican goes unpunished by a Queen's court. So I admit no "previous convictions". I admit only previous miscarriages of justice and wrongs done to me at the heavy hands of the Queen's courts' officials. So I don't expect that there will be a fair trial for me, nor for any republican, in any unjust royalist kangaroo court of this kingdom, where judges, who serve the Queen but not the people, will be sitting in judgement on republicans, who serve the people but not the Queen. Therefore in the unfair show trial on 4th November I will be appearing before another royalist court which can so easily do a wrong to me, especially if such court-wrong-doing is thought by wrong-doing royalists to serve their Queen. I believe that there can be - courts which serve the people and do what is right and just, or, courts which serve the Queen and do what is wrong and unjust but, in my republican opinion, there cannot be such a thing as "a court which serves the Queen and the people and does what is right and just, all at the same time". In serving the Queen, royalist judges often follow misleading evidence lead by "the Crown" - the prosecutors defer to the kingdom's fallible authorities have contempt for human rights law dish out cruel punishments for trivial or minor offences and so do wrong to the accused and a disservice to the people and therefore it is time to end the status quo of royalist courts, pretending to be "courts of justice" which royalist courts realistically can never be. No doubt my lawyer will do his best on the day but I believe that my best political defence can only be published by myself, in my blog, in emails, in press releases and in this Political Forum post. Scientists for Freedom of Expression in Scotland Peter Dow Peter Dow on Indy-Ref day, 18th September 2014 Peter Dow, B.Sc. Hons. (Edinburgh) Former lecturer in Computing and Mathematics, Glasgow College of Nautical Studies. Independent research in applied science. Author - political, economic & social science Politics - Internationalist. Republican Socialist. Websites - "Scottish National Standard Bearer" SCOT.TK "For Freedom Forums" FIGH.TK Twitter @ peterdow Police quote political tweets as pretext for raid of Peter Dow's Aberdeen home in July 2014. Computer with irreplaceable science data seized "not like Gestapo" claims a detective constable Prosecutor trumps-up ridiculous charge of "threatening communication" and court grants bail conditions limiting Dow's access to websites Flimsy case demolished in 8000-word email reply Jon Godwin Jon Godwin Professor Jon Godwin, MSc DPhil (Oxon) CPhys MInstP FRAS FRSS Reader in Statistics, Institute for Society and Social Justice Research, Glasgow Caledonian University. In emails to Peter Dow, Professor Godwin writes - "I should of course share your deep upset at having my research and the "tools of my trade" seized from me by the powers that be. ... what I might be able to do to help?" "... commiserating with you over what seems a quite extraordinarily high-handed reaction to it, in particular considering the sometimes very colourful conversations one encounters daily on internet bulletin boards, etc etc. In particular, seizing your property in "evidence", rather than perhaps just copying whatever might be relevant to the possible case and then returning it, seems almost wilfully obstructive and I can only imagine your consternation as to what might become of it later. ..." "the implications for "freedom of expression" are potentially serious. Meanwhile, I wish you well and hope that this matter ends happily." - Professor Jon Godwin, Glasgow Caledonian University, January 2015 Contact - Peter Dow, 21 Hollybank Place, Aberdeen, Tel. 01224 583906 WANT TO HELP? If you would like to help my political defence then here are some things you can easily do - Suggested tweets Please copy and paste these texts and tweet them! and or post a similar tweet but with a hash-tag list of your own composition. Post a link Please post a link to my political defence blog on Facebook or on another social media network or on an on-line discussion forum of your choice. Thank you very much!
-
After I started this topic, I have since found another trochoids interactive demonstration webpage, this time by Christopher J. Henrich. His code is in Javascript which means it is pretty much open source, can run on most modern web browsers and therefore is ideal for me to modify. So I've made a start and I'm publishing a webpage today which partially performs some of what Tony Kelman's demonstration does. I've a lot more to do yet but if you want to see how far I've got and monitor my progress, then click to my webpage using the following link. My page includes links back to Christopher J. Henrich's original webpage and he is OK with me publishing this link. Anyway see for yourself. Mathematics of the Wankel rotary-engine shapes Webpage by Peter Dow
-
Regarding the mathematics of the unusual shape and profile of the Wankel engine triangular rotor and combustion chamber housing, I'm reviewing a mathematics demonstration I have just come across but which has been on the internet for a few years but, like me, you may not have come across it before now. "Wankel Rotary Engine: Epitrochoidal Envelopes" by Tony Kelman on the Wolfram Demonstrations Project. http://demonstrations.wolfram.com/WankelRotaryEngineEpitrochoidalEnvelopes Review by Peter Dow If you think this video looks interesting, I highly recommend that you download the Wolfram CDF player software so that you can experiment with the features of Tony Kelman's demonstration. To quote Tony So selecting reference frame = epitrochoid allows the display of the familiar KKM Wankel engine and selecting reference frame = fixed centers shows Wankel's original DKM engine with rotating housing. You can slow the rotation animation down as well.. Looking at eccentricity ratios widely different from what we see in real Wankel engines is quite a revelation too. As if all that wasn't enough, you also get to download and look at Tony's open source code and in particular the maths equations he uses to generate the curves. Tony suggests some extensions to his demonstration. Well I have ideas of my own - I'd like to see computations of the areas between the curves representing the combustion chambers and a calculation of compression ratios for example. Unfortunately, I don't have the Mathematica developers software package which, unlike the free player I got to view the demo, you have to pay - A LOT - for. Excellent demonstration! Can't praise it highly enough!
-
Your argument is like saying "Without roads allowing people to drive cars, buses and lorries around cities, transport in cities would be impossible because cities are low-vehicle environments (hypo-vehicular)." No, cities are not "low vehicle environments". In fact they are well saturated with vehicles. By means of that analogy, I hope to make the point that yours is a misleading way of talking about all the oxygen which is available for the cells in our bodies. If you went around saying that cities were "low vehicle environments" they may not have you carted away to the funny farm if you were lucky but you'd find it very difficult to hold down a job teaching urban transport planning anywhere talking such nonsense. Yes there are some places in cities where cars can't get to - like there are some places in our bodies which oxygen can't get to. Overall though, the picture is of cars in cities and oxygen in our bodies. Cities are not low-vehicle environments and bodies are not low-oxygen environments. Obligate anaerobe bacteria seem to be most promising for the bio-agent task. Like I explained earlier, the reference strain of bio-agent is kept in a laboratory, where all kinds of strains of bacteria can be stored separately and keeping non-drug resistant strains away from drug-resistant strains. You simply run the laboratory well enough so that some idiot does not mix up the batches of one strain with the other strain. You put labels on the petri dishes saying things like. "DANGER! Drug resistant strain - do not use as a bio-agent!" Or you keep the drug resistant strains in another building because you can't trust the fools you've hired not to mix them up if they are stored in the same building. Is this so hard for you to understand? This has nothing to do with the development of drug-resistant strains of bacteria in the population. That's a separate issue. My treatment approach has nothing to say about the issue of drug-resistance because the bio-agent is not selected by taking samples from anywhere other than strictly controlled science laboratories and the lab would supply a strain which was not resistant to the anti-bio-agent drug it was paired with. If I want a drink of water I drink from the tap, I don't drink from the rainwater in a puddle on the street. I choose the pure sample of water. Likewise with the bio-agent, the doctors would choose the pure strain which presumably would be supplied by big pharma, along with the anti-bio-agent drug. Doctors would not go hunting for bio-agents themselves same as they don't go hunting for anything else they use in hospitals! Doh! Is this point so hard for you to understand? No that's not correct. I did mention use of an antibiotic in the this paragraph from my OP. Now maybe the penny did not drop for you that I was talking about an antibiotic when I used the word "anti-bio-agent drug"? It looks like I did not use the word "antibiotic" until my post #26. But I was always talking about an antibiotic when I used the word "anti-bio-agent drug". But, specifically I was talking not about just any old antibiotic picked from the shelf at random but one selected for use as part of the pair of phase one treatment tools - the bio-agent and the anti-bio-agent drug (maybe supplied as a twin pack by big pharma). Is that clear for you yet? Well the idea would be to saturate the body with too much bio-agent for the immune system to mop up before the bio-agent got its spores or whatever so widely distributed that the body could not stop the spores germinating in hypoxic cores in due course. But that'll be a spread of the inactive form of the obligate anaerobe - that doesn't mean a wide-spread living infection that is harming the body and which the immune system, or you on the patient's behalf, needs to be too worried about. I do understand the topic. I also know that others do not understand me. That's a communication problem. I am working on it, but it is not easy. No "sepsis" means a different kind of "overwhelmed" immune system. Sepsis means a very active immune system responding to what is perceived by the immune system to be a rampant, very severe infection. In my approach, the distribution of a large enough number of spores etc. around the body does not mean a severe infection. It will be a mild infection with a fairly harmless anaerobe. Now, of course there is always a danger of an over-active immune system. Some people have allergies and some people might develop an allergy to the bio-agent spore, if indeed spores are used. OK so there is a job for the intensive care to manage an inappropriate immune response - using anti-histamines or whatever. It's manageable. Well I've always had difficulty explaining what for me are simple matters to the less gifted. It is very frustrating for both parties no doubt and thank you for your patience. I've answered this point recently in post #65 in reply to Ringer. Well the bio-agent can only thrive by killing and consuming human cells and debris where it is hypoxic, where those human cells cannot respire aerobically, where the bio-agent must respire anaerobically. In its inactive form, the bio-agent is spread around the body yes. But it is only activated where the local environment is hypoxic, and that's not where the living cells are. Precisely, "in the right conditions" and those conditions only apply so far as the bio-agent is concerned, in hypoxic tumour cores where a large feast of easy meat is awaiting the obligate anaerobe to dine on. Quite. I do understand. I think you understand the reality of the body as well but your choice of language at times I find to be inappropriate and not helpful.
-
Yes I knew that already but thanks for the etymology lesson anyway. Well cancers vary a lot and some do grow faster than the body can sprout vessels to supply the tumour and those are the only tumours which have hypoxic cores, other tumours don't, correct. Phase 1 treatment is only intended to treat hypoxic tumour cores, cores that are properly hypoxic and where cancer cell division has ceased because there's not enough oxygen to divide. Right from the OP, phase 1 was never intended to treat "marginally anaerobic", slightly hypoxic tumour cores or tumour cores with good blood vessel supply. Right from the OP, the limitations of phase 1 were made clear that it was never intended to treat the rim or periphery of any tumour or the whole of smaller tumours which will be well oxygenated because they are so small that oxygen can get into the middle of them, even if they haven't grown their own blood vessels. If I had thought for one moment that phase 1 was a complete cure, I would not have bothered with a phase 2. Phase 1 is guaranteed to achieve phase 1 goals as advertised, no more, no less. Woah there; steady on! From that Clostridium perfringens Wikipedia article you linked to That's when gangrene is a problem because a major trauma, like having parts of your body pinned under something heavy for hours or getting shot in war, causes a massive quantity of your body tissue to lose its supply of oxygen and that is indeed a problem for the oxygen-deprived tissue - it is called ischemia - Wikipedia: Ischemia which becomes an opportunity for anaerobic bacteria. So muscle needs to be ischemic for an anaerobic infection to take hold in that muscle in the first place. No ischemia, no gangrene. It's not the case that if you inject a strictly anaerobic bacteria into healthy tissue that the anaerobes can cause an infection at that location. No; healthy tissue is too well oxygenated for anaerobes to proliferate. So they'd just be dormant, just stuck in place doing nothing or circulating around until dealt with by the immune system. It's different in ischemic tissue and it is different in hypoxic tumour cores. Gangrene needs ischemic tissue to get started. It can only spread from where it has established a large "base of operations" so to speak, where large quantities of tissue are hypoxic, ischemic, necrotic because some injury or disease state has blocked off the blood supply to those parts of the body. In order to spread into healthy tissue the anaerobe needs to kill the healthy tissue from outside it and the only obligate anaerobes which can do that have very lethal toxins which large bacterial infections can make enough of so that when the toxin seeps into the neighbouring healthy tissue there's enough toxin to kill the healthy tissue and so the infection can spread. Now for use as a bio-agent in phase 1 you'd pick an anaerobe that didn't have a very lethal toxin, maybe make a genetically-modified anaerobe, like Clostridium novyi-NT, which didn't have that ability to kill healthy tissue from outside that healthy tissue. Then you'd also have the anti-bio-agent drug to moderate the infection, reduce the activity of the bio-agent so that any toxins it was making were being made in such small quantities that they were easy for the body to dispose of safely. Well the fact is most of the body consists of living body cells and where they are, they have oxygen thanks to the blood and these critical areas are not somewhere the obligate anaerobes can proliferate. If an obligate anaerobe can find some nook and cranny of the body which is hypoxic enough to activate and is lucky enough to find enough resources located at that nook and cranny to become active in tiny numbers that's no big deal because an obligate anaerobe still has the problem of finding a further food source to proliferate. There isn't that much of the body normally, that doesn't have oxygen enough to deactivate obligate anaerobes. So they'd be stuck active in that nook and cranny and maybe sending a few spores out now and then but not proliferating significantly because they can't. They are surrounded by oxygenated tissue and that pens them in. If a good selection of bio-agent is made gas gangrene would not be the problem you claim. If with some patients who already have ischemic and nectrotic tissue because of some other disease, or perhaps the cancer tumours have blocked blood vessels to other parts of the body then yes, of course, then there is more of a risk of gangrene in those cases but that threat is more likely from other anaerobes, the ones like Clostridium perfringens most commonly associated with gangrene, not from the bio-agent which is selected so that is doesn't find it easy to spread to healthy tissue. So some cancer patients do get Clostridium infections and gangrene and some die from it but that's usually down to inadequate medical care. I'd prefer to phrase it this way - the body cells are not hypoxic thanks to the functioning of the circulatory system. ... and all of the cells of the body are well saturated with oxygen and not hypoxic, not in the least low in oxygen. Ah at last - a different question. How refreshing! The development of drug-resistant strains of bacteria depends on those strains being able to keep themselves going by spreading from patient to patient. The bio-agent reference samples will be stored in an isolated laboratory and will not be mutating in vitro in the lab and if any samples ever did, they'd be disposed of. The bio-agents to be used will be bred from the reference samples. They won't have time to mutate in-vivo before they are killed off before phase 2. In any case, if a patient jumps out of his bed after phase 1 goes home and in 20 years the bio-agent in his body has mutated to a drug resistant strain it matters not because we won't be breeding bio-agent from the bacteria in that ex-patient but from the reference samples in the laboratory. Your concern is as logical if you buy a pure bred puppy from a dog breeder but you are worried that other dogs might have escaped from the dog breeders kennels and have bred with other stray dogs to produce mongrels, not pure-breds. Well, so what, so long the puppy you get is a pure-bred you should be happy so quit your whining. I should explain things better. Millions of lives are depending on that. Still mixing up your phases I see. No, the immune system is not eliminated; it is not even weakened in phase 1. It's there full strength to help to contain the bio-agent. Well I am re-working and adding useful examples as I go along. The first OPs I posted in science forums were somewhat rushed and inadequately presented because I was eager to share my "Eureka" moment with you all and hadn't taken the time to research the answers to some important questions I had, like a few type H drugs are indeed available now used as "growth factor receptor inhibitors". I did say that but that was in response to someone claiming I was looking for, can't remember the exact words, something like "magic" bacteria, whereas, no, it is simply selecting the best for the bio-agent job which are available from obligate anaerobes, whether native or genetically-modified strains. The point I was making was that what is required for the bio-agent is not some mythical beast but the most suitable out of what is there and so by all means pick an existing genetically-modified strain like Clostridium novyi-NT if tests prove that to be the most suitable when compared with the 100s of native obligate anaerobes out there. I was just making the point that the behaviour required from the bio-agent desired is characteristically typical behavior, not at all science fiction. I am now including a link to Wikipedia articles about Clostridium novyi-NT in the latest versions of my OP posted elsewhere because that often comes up in discussions, but my approach is in no way founded upon that GM strain, as if the approach would fail without that strain. I don't misunderstand. Otherwise you'll fail your students as heretics and they won't get a job maybe. OK, but you are still twisting the reality to fit your dogmatic point of view - "the body as a hypoxic environment". A dead body yes. It's more complicated than you say. Oxygen saturation varies from point to point in the body, it's is not a strictly uniform O2 saturation everywhere but human cells respire aerobically in the body and to be able to do so then immediately outside each of those cells must be an oxygenated environment - the extra-cellular fluid must have good oxygen saturation for the cells to respire aerobically. That's an important fact which you are obscuring with your "hypoxic body environment" dogma. Maybe we should agree to disagree on our respective use of those words because I don't think either of us is going to change our minds or our language. I know I am not.
-
Well I have been consistent from my OP that not all types of cancer will respond to phase 2 treatment. I'm not chopping and changing my story. The issue is whether the cancer cells divide more in response to typical growth factor signalling. Let me give an example or two. Example 1 - cancer can be treated by phase 2. Before treatment with type H drugs Normal cells of tissue type X divide once every 4 days and the number of them stays the same because new normal cells replace the normal cells which have died Cancer cells of tissue type X divide once every 2 days and the number of them grows because there are more new cancer cells than any cancer cells which might have died So in that case the same body cell signals make the cancer cells divide at a faster rate than normal cells, every 4 days for normal cells, every 2 days for cancer cells. That's a cancer simply because the cancer cells are dividing at a quicker rate but not dying at a quicker rate During treatment with type H drugs Normal cells of tissue type X have stopped dividing thanks to type H drug Cancer cells of tissue type X still divide once every 2 to 3 days despite type H drug which only has a small effect to slow their division but the cancer cells are killed by the type K drug when they divide so, so after 3 days all the cancer cells are dead but the treatment lasts for 4 days just to be sure to kill all the cancer cells Example 2 - cancer cannot be treated by phase 2. Before treatment with type H drugs Normal cells of tissue type X divide once every 4 days and the number of them stays the same because new normal cells replace the normal cells which have died Cancer cells of tissue type X divide once every 4 days and the number of them grows because none of the cancer cells are dying So in that case the same body cell signals make the cancer cells divide at the same rates as the normal cells, every 4 days. That's a cancer because those cancer cells are all immortal, they don't die like they should, ever. During treatment with type H drugs Normal cells of tissue type X have stopped dividing thanks to type H drug Cancer cells of tissue type X have stopped dividing thanks to type H drug Type K drugs don't kill any of the cells. No. We have the kind of drug which can block growth factor receptors in some tissue types already. Wikipedia: Growth factor receptor inhibitor So the type of drug is not "hypothetical". We just need more of that type of drug for other tissue types, other growth factor receptors. That's something well within the abilities of big pharma to deliver eventually. That science is known about. So my approach whilst not "easy" can be realistically planned for. We don't have any kind of drug which can force apoptosis in every cancer cell but leave all normal cells alone, I think. That science is unknown I think and I am fairly sure no such drug is currently being sold for treatment. It is not realistic to plan any approach like that before anyone has demonstrated a drug which forces apoptosis and treated some patients with it successfully. If such a very useful drug could ever be demonstrated then yes then it would be possible to plan an approach for that but I don't think it has been demonstrated. So my approach would be a lot easier. I know exactly how my approach would work with the types of cancer where it would work well and some ideas of what to offer where it doesn't work so well - maybe just in phase 1 will it do much. So it is not a cure all. I never said it was. I said it wasn't.
-
I think you'll find that I have responded to all previous posts which are making scientific points. Patience please. I am now responding to post #30 and the newest posts are numbering around #53. You may feel ignored but it is simply that there is a queue to be processed. So I am a long, long way behind with the backlog of posts to reply to and you'll just have to wait until I have time to post my replies which will usually be in the same order to the order which the posts I am replying to were posted. So you are really asking about how practical treatments lasting for weeks, on and off, are? It is just that you quoted Ringer asking about curing treatments in only a week but your question didn't ask about that, but about longer treatments. So you haven't made it clear whether you expect me to explain further about that point. Anyway, briefly on the first point, more aggressive treatments are easier to cure because the cells are always dividing and so you don't have to wait long to kill all the cancer cells. It is the slower-growing cancers who cells pick and choose their time to divide that require a more extended treatment regime. Anyway back to your question John, it is not meant to be funny and my approach is aimed at reducing the tragedy of so many cancer deaths. Well if a full recovery can be made in a few days, building up the patient's strength, especially as regards those rapidly dividing cells, then the expectation is that the patient would be more healthy, not less healthy, at the beginning of each week on, compared to the beginning of the previous week on. What you seem to be forgetting is that if the patient stops taking the drugs then the suspension will stop, the cells will resume normal division. This is a treatment wherein because it is only cancer cells that are being killed so then the recovery is very rapid, unlike say with bone marrow transplants now when a lot of normal cells which were dividing when the chemotherapy was done, were also killed at the same time. That chemo takes a lot out of the patient and recovery is slow. My approach spares the patient that long recovery time. Your link only supports the notion of multiple drugs regimens, not phased treatment plans. If you can come up with a link which shows a phased approach, bio-agent / bacteria in phase 1 followed by chemotherapy in phase 2 then I will concede your point but only if you find such a link. I don't know of one. This is my approach described here. Not someone else's. This could be new, I don't know of anything the same but you never can be sure. It works like this and in the following sentence "H" stands for the use of the type H drugs to stop normal cell division but leave cancer cells still dividing and "K" stands for the use of type K drugs to kill all dividing cells Ready? OK If H works then K kills only cancer cells. If H doesn't work then K kills both types of cells So if you understand that short summary then you ought to understand that my approach works if type H drugs work as advertised. Got it yet? Questions can be hard enough to answer without having to guess at the context the poster was thinking about but was too lazy to actually type in. No, that's almost entirely wrong. The entirety of the living human cells in the human body experience a suitable oxygenated environment to allow them to use aerobic respiration. Now sure, you could have parts of the body with no human living cells there and at those places alone there the oxygen levels could be hypoxic, maybe. Certainly, if the human is not happily breathing air, if the body is injured and the blood flow is obstructed, not getting oxygen to some cells - sure then hypoxia is certain. Look Ringer, aside inside from our digestive tract and inside the bladder where the urine is, where can you find a single cubic inch of the healthy human body which is all hypoxic and what is there at that place for anaerobic bugs to eat? I don't think you can name such a cubic inch but make my day. Cancers must be of the living digestive tract cells which have blood vessels supplying them oxygen same as most other cells do. It is only the inside of the digestive tract - which many anatomists would describe officially as "outside the body" (kind of strange way to look at things I know) - it is only inside the digestive system and inside the bladder too where there is much of anything which is hypoxic. Well what I am finding is that chemists don't know their biology and biologists don't know their chemistry and the doctors are in the middle of this watching the scientists battle it out and trying to be helpful! Well I would say curing cancer is the reward and my treatment has fewer dangers. Well the bio-agent won't be killing anything inside the gut, nor is it supposed to. That's not where the cancer is. Ah you are mixing up your phases. The bio-agent is only needed for phase 1. After phase 1, the bio-agent is killed off using a large dose of anti-bio-agent drug. Before phase 2, the gut flora need to be killed off as well. So yes the immune system is an issue but a manageable issue. Sorry what was the question again?
-
Drugs of the growth factor receptor inhibitor type my approach requires to be used as type H or "Halt cell division!" drugs have already been made, so it's a reasonable expectation that other drugs of that type could be made. It should be very useful for cutting edge medical science researchers and big pharma out there when I explain precisely how my approach can use that type of drug to cure cancer in a different way from how such drugs are typically used today so that their efforts can be directed in the most efficient way. I'm showing them the way and the path to a cure. That means we'll get there sooner. Oh manufacturing more of the same bacteria which already exists is trivial. They reproduce themselves given a suitable foodstuff to feed on. What's not so easy is to modify genetically a species of bacteria so that you can manufacture a bio-agent that's ideal for a particular application. However, medical science researchers have managed to produce a genetically-modified strain of Clostridium novyi, the "NT" strain to be less toxic for use in bacterial treatments of cancer tumours. Wikipedia: Clostridium novyi - Clostridium novyi-NT - Potential Therapeutic Uses in Cancers No, my expectations are reasonable, for the bio-agent and the drugs my approach needs. Not exactly, no. The organisms under consideration for use as a bio-agent are known as obligate anaerobes. Wikipedia: Obligate anaerobe So it would be more accurate to say the properties of the anaerobe are It eats human or other cells or cellular debris in a hypoxic environment. It doesn't eat anything in a well-oxygenated environment Those properties make obligate anaerobes useful for eating those cancer cells which happen to be located within some tumour cores which are hypoxic because the tumours have outgrown the blood supply. Their properties as stated by me, not you, yes. As stated by you, because you didn't state their properties accurately, no. No, it matters a lot. Human cells are more similar to fungal cells at a molecular level, unlike bacteria which have taken a quite different evolutionary path. Wikipedia - Antimicrobial - Antifungals This means in general terms that it tends to be easier for bio-medical science to come up with an anti-bio-agent drug which kills the bio-agent selectively but doesn't harm the patient if the bio-agent is a bacteria and not a fungus. So a fungus would be a bad choice of bio-agent for that reason. Well it is not so John. You need to think about this a bit more. The sort of bio-agents and drugs I need for my approach are real enough. We may not know which anaerobe would be best, we may not have all the growth factor receptor inhibitors available today to implement my approach but the possibility that suitable bio-agents and drugs could be sourced is real. Now even though it is a real possibility that they can be sourced eventually that doesn't invalidate me explaining why they should be sourced as soon as possible, so that we can cure cancer as soon as possible.
-
Abstract A new 2-phase treatment to cure cancer is proposed. Phase 1 would use a live bio-agent paired with a moderating anti-bio-agent drug to target and kill hypoxic cancer tumour cores. Phase 2 would employ 2 drug types - firstly a mixture of drugs of the growth factor inhibitor type, some (perhaps most) yet to be developed, would be required to halt selectively all normal cell division but not halt the characteristically aberrant cancer cell division and secondly, conventional chemotherapy drugs would be used to target and kill only the dividing cancer cells. Update - Wikipedia: Growth factor receptor inhibitor
-
In general terms, I'd expect my approach to be significantly safer than any current therapy which uses chemotherapy (or radiation) to kill all dividing cells in the body. My approach only involves putting cell division of normal cells on hold, not killing off the dividing cells. Therefore the recovery after elimination of the drugs from the body should be very quick, not many months like it can be after a bone marrow transplant. Unfortunately, my approach is not easy because it is not easy to source the type H drugs that halt normal cell division but allow cancer cell division to proceed in character. It's a challenge, especially if the patient's immune system is compromised for months after treatment when the intensive care against infection requires to be extremely vigilant for just the reason you state. The advantage of my approach is there should be no such long intensive care required after treatment, only during treatment. Correct. Again with my approach that's a battle that is easier to win because the battle is over quicker and the army of medical resources required to wage the battle against infection only need to be deployed on the battlefield for a shorter time. I've often found it curious how big pharma can get away with a claim that an antibiotic is "broad spectrum" if isn't quite broad enough to kill the Clostridium genus? The answer, I would have thought would be to include an antibiotic which is good against Clostridium infections within the "broad spectrum" antibiotic dose in the first place? No? Is that too obvious a solution? In my approach, blood transfusion, reintroducing stored quantities of the patient's own blood can be done if required. It occurs to me that the stored blood may contain floating cancer cells so it too would have to be treated with the type H and type K drugs in-vitro before being cooled to maintain its shelf life. Again a problem which is moderated when the patient's skin and mucous membrane cells start dividing again after treatment. Clarissa, your contribution has been most to-the-point and welcome. Thank you very much. The risks are real but manageable I contend and whilst not dismissing those risks, the bigger issue for me would be sourcing the type H drugs required.
-
Not at all. Not "unclear" to all professional biologists I trust. I am presenting a sound argument that survival with intensive care would be possible. Evidence requires experiment with those type H drugs which are not all available to block all cell division. The argument would be that if a patient can survive without cell division of each type of cell for a time, then one can reasonably assume that the patient would survive the cessation of all types of cell for a time. Consider the use of epidermal growth factor receptor inhibitors in clinical applications. The patients survive the cessation of epidermal cell division. I argue that there is no cell type which if it ceases dividing must inevitably cause the death of the patient so long as suitable intensive care is given. You seem to be expecting or demanding evidence of the success of a proposed treatment that it would work - at the earliest proposal stage, before the drugs are all available to test, before experiments with animals have been done. You want evidence before the experiment is done. That's not very scientific. When President Kennedy said "We choose to go to the moon in this decade and do the other things, not because they are easy, but because they are hard" the sceptics demanded evidence that those hard things could be done, before they were done. They scoffed at Kennedy because he had no evidence that sending a man to the moon would not kill the man. Now how foolish do they look? Your links don't make your point in a way that is useful to me. Perhaps if you were able to copy and paste the relevant sentence or two from your links that would help me a lot? It's a proposed treatment with adverse side-effects, yes, which would require intensive care, of course. I apologise if I have offended you. I don't do "gracious" at all well. If you want gracious I'd refer you to Condoleezza Rice. If you want a cure for cancer you've come to the right place. Well the other obvious factor is that blood is the easiest body part to repair or replace in medical practice. Blood transfusions are a trivial medical intervention these days. A patient could donate his own blood before treatment and have it stored for transfusion if that was necessary. It's only the red blood cells that last so long though and the much shorter life span of white blood cells would be more of a concern admittedly. Quite but I was pointing out that the 6 to 16 window suggested by the reference offers plenty of time for the treatment drugs to kill the most aggressive cancers whose cells are rapidly dividing more frequently than that time-scale. Incidentally, Wikipedia suggests a much longer life-span for macrophages of several months. Well new macrophages could be sourced from monocytes in transfused blood as necessary. Understood. On the other hand, if facing a terminal cancer disease, a cure with risks is worth taking.
-
It appears that what I have referred to as "Type H drugs" and "growth factor blockers" look to be my redundant names for "growth factor inhibitors" (half a million hits on google!) and "growth factor receptor inhibitors". (700,000 hits!). Though I note that "growth factor blocker" and "growth factor blockers" appear to be getting hundreds of thousands of hits now too - I thought I had tried that search term earlier and got nothing, maybe my typo or some problem with google?) Wow, 1.8 million hits for "growth factor receptor blockers"! {Those are hits with the quotes included in the search term so those should be hits for the exact phrase. Sorry but my google links were playing up and I've removed them so you'll have to use your own initiative, perhaps copy and paste the search terms into your search box} Inhibitors / blockers - same difference so I am content to use any of the names "Growth factor inhibitors" or "Growth factor receptor inhibitors" or "Growth factor blockers" or "Growth factor receptor blockers" from now on for this class of drugs. So that's actually very encouraging for the early adoption of my approach to cure cancer because the drugs needed are not as "unknown" and "do not exist", as a class of drugs, after all. That's not to say that all such growth factor blocker / inhibitor drugs which would be needed for the successful adoption of my approach are now available but it looks like some are available and hopefully the rest will be made available eventually. I've found this wikipedia link - EGFR inhibitor - redirecting to - Epidermal growth factor receptor - Clinical applications There doesn't yet seem to be a general Wikipedia page for "Growth factor inhibitor" or "Growth factor receptor inhibitor" or "Growth factor blocker" or "Growth factor receptor blocker". So that's something for me and other Wikipedia editors to think about coming up with. If we can at least start talking in a structured way about this class of drugs then that'll be progress.
-
"Most" by what measure? By the measure that counts - living human cells, most of the body is oxygenated by the circulations and our cells respire aerobically for the most part. Do you mean the most number of cells, including within the total the gut microbe cells which exceed in number human cells, are in an anaerobic environment? That would be the only measure I can think where your "Most" would be true. I'm not conflating the two but I can re-write any sentence of mine to make that appear more obvious to you if that's what you need? So re-writing the sentence you quoted - I don't see any flaw in the idea that a suitably selected anaerobic micro-organism would thrive, flourish and grow at the expense of all human cells in hypoxic parts of the body. How's that for you? Happy now? I understand. Well to be pedantic I haven't even insisted that the bio-agent in my approach must be a bacteria, as opposed to some other anaerobic micro-organism. What I have insisted upon is that whatever obligate anaerobe is selected it must be selected as one of a pair of phase 1 agents, paired with an anti-bio-agent antibiotic to which the bio-agent is very vulnerable. So the possible impact of an uncontrolled infection is a danger which has never been dismissed in my approach. Rather controlling and moderating the infection is planned for in this approach. No other reasonable interpretation of my OP is consistent with what I have written. As someone with a lot of posting experience in forums I have become accustomed to somewhat unreasonable misinterpretations of what I have written. The difficulty with that claim is the treatment regime would be able to add a sufficient amount and rate of bio-agent to the body so as to make the immune system's job slightly more than trivial because of the sheer numbers of bio-agents that were being added to the extent that the immune system would be unable to isolate and eliminate from the body all the bio-agent before the bio-agent establishes itself in the target hypoxic tumour cores. Once established in the hypoxic tumour cores the bio-agent is protected from a trivial immune elimination by the hypoxic environment. I welcome feedback and as far as genuine limitations are concerned I am happy to acknowledge those though as far as the readers perceived limitations which are founded on nothing more than misconceptions and misunderstandings of my approach are concerned I hope to show that the fallacy of such so-called "limitations". No I haven't stated that. Either native or bio-engineered bio-agents can be considered. I've even quoted an example of a bio-engineered strain of Clostridium novyi - "NT" strain - as a promising candidate for use as a bio-agent in phase 1 of my approach. Well the toxicity of anaerobes really depends on them being able to produce toxin and that's a function of the anaerobe having both a suitably hypoxic environment and a food source which they can metabolise into toxin. Simply injecting lots of bio-agent which has a theoretical ability to generate vast amounts of lethal toxin into the body doesn't automatically serve up for the bio-agent an environment in which the bio-agent can make their characteristic toxin in lethal or even systemically significantly amounts. It really works the other way around. The body has to be dead or injured before its organic resources become "easy meat" for the bio-agent. The only easy meat on offer is the hypoxic cores of tumours and yes those could be converted eventually into an amount of toxin which would be lethal if administered in one dose but the approach is to limit the rate at which any toxin is produced by use of the anti-bio-agent antibiotic down to levels which have no toxic effect on anything but the tumours concered. Then I wonder how your fellow anatomy 101 students will react to your claim that "Most of the human body is an anaerobic environment."?
-
No because I brought my own ideas describing a new approach to cure cancer to this and other internet forums and I've been willing to explain my ideas to help get them understood sufficiently by others to allow that new approach to be implemented in due course Well the bacterial treatment concept has known limitations, of infection control and only effecting hypoxic tumour cores, which renders typical such treatments a) unpredictable and b) not a cure The novelty of my approach is to explain how a bio-agent treatment can be a) moderated using an anti-bio-agent antibiotic to render the treatment more predictable and b) used as phase 1 of a cancer cure which requires a new phase 2 treatment using a new type of drug I am proposing which would be used to halt normal cell division during the 2nd phase of treatment. It's like, when someone invented the swept-wing jet-powered air plane to fly a lot faster than a piston-engine plane with straight wings, someone like you came along and asked "How is that novel because your plane uses wings and wings already exist?". Yes wings had been around but swept wings with a jet engine gives faster flight. Just because a designer is using existing ideas and building and improving upon them as part of his new design approach, that doesn't mean that the designer isn't doing something novel. That's not a problem, that's evolution's solution to a problem. The anaerobic bio-agent would be no more lethal than the multiple species of anaerobes which already live in the digestive tract and they can't even eliminate each other or breach the gut wall. I am presenting a clear enough overview of the relevant mechanisms for the relevant research scientists, professional pharmacologists and oncologists to be able fill in the details as and when required. There are many medical treatments which require intensive care to successfully complete - organ transplant is one such. Wikipedia - Gut flora So those "internal bacteria" in the gut have nothing to fear from the bio-agent which is likely to be simply one of their number conscripted to act as a bio-agent in other parts of the body. However, the bio-agent is not injected into the gut where there are useful flora for us to worry about. The bio-agents will be injected into the systemic parts of the body which are routinely sterile and where and when they are not sterile have a very active immune system pursuing pathogens, killing them, walling them off and so on. The nomenclature of "Type H drugs" was chosen because H stands for "Halt cell division!". Another useful name for them might be "Growth factor blockers". I was talking about those cancer diseases when the body's defences have failed to halt the uncontrolled division of cancer cells. This may not be a true or accurate description of some cancer diseases where the cancer arises not from a failure to control cell division, which remains at normal rates for that type of cell, but rather a failure to control the death of cells via a damaged apoptosis function. Well I haven't done all that work. That comes later and it won't be done by me alone. I'm just providing the approach and a lot of those details need other scientist and engineers to work out. Yes I do know that. Only for those patients whose cancers have cells which are rapidly dividing, whose cancer cells divide every few days. For those more aggressive cancers the cure is more rapid. For slower growing cancers you have to keep the treatment going for longer, perhaps have treatment on, treatment off weeks, waiting for the opportunity to catch and kill each cancer cell as it divides.
-
No that's not how I have defined the bio-agent's properties. Not at all. You are confusing my description of the clinically desirable outcomes of using the bio-agent, what the approach's goals of treatment in this phase 1 are, with the bio-agent's natural behaviour causing unwanted side-effects which I've always acknowledged. You seem to be refusing to accept that I am acknowledging, have always acknowledged, right from the OP that unwanted side-effects would be expected to be observable and measures must be taken accordingly. Of course there would be an expectation that other bits of the body which are equally as vulnerable to the bio-agent would suffer the same kind of attacks from the bio-agent. The approach would be to expect a tendency for there to be side-effects and to manage the infection with the anti-bio-agent antibiotic drug which is integral to phase 1 treatment so as to reduce the systemic side-effects and local side-effects on particularly vulnerable sites in the body right down to acceptable and tolerable minimal side-effects. Well let me supply another better analogy. If, hypothetically, I go online to a nuts and bolts website and ask them if they have a nut to fit an old bolt I need a nut for that I can describe the dimensions of and if they don't have such a size of nut already if it is a good website they will accept a custom order from me to make the right size of nut to fit my bolt. The order is meaningful. Of course if it was your nuts and bolts website you'd refuse to do custom orders and you would say - "ah but you just wishing that that size of nut existed isn't meaningful". My wish for a nut of the right size would be meaningful. But it would not mean anything to you maybe because that's the kind of poor service that you would offer. You don't ever do custom orders. If it is not on your shelf already then you don't even want to think about it. That says more about you than it does about me wishing to source a nut of the right size. I'm not asking for a warp drive. I am asking for a pharmaceutical drug which is a chemical equivalent of a nut to fit a bolt. OP does not neglect general limitations of bio-agents. You neglected to notice that OP describes 2 phases and 2nd phase (new kind of chemotherapy) works on parts of tumours that 1st phase (bio-agent) doesn't work on.
-
Ringer Oh my approach doesn't require "modifying" bacteria. My OP didn't mention "modification" of bacteria to do anything other than what comes natural to bacteria. Yes it is true that a bio-engineered less-toxic strain of Clostridium novyi - the so called "NT" strain - has been mentioned in quotes during the discussion in this thread - and I don't have any evidence to dare to dispute the researchers use of NT strain as better suited to the native stains for any such bacterial treatment of cancer tumours. If strictly or obligate anaerobic bacteria are used for this they could only ever attack organic material of any kind which is situated in hypoxic areas of the body where they can come to life from the inactive spores. Ringer The "anaerobic thing", as you put it, is everything. The approach uses strictly or obligate anaerobic micro-organisms which are deactivated when there is oxygen in their environment. If you want specifics - Wikipedia - Obligate anaerobe Ringer 3 types of drug are used. 1 type in phase 1 and two types in phase 2. Ringer Phase 1 may imply the selection of an anaerobic bacteria to use as the bio-agent. Ringer I haven't mentioned using viruses so I don't know where you got that from? Ringer In phase 1, the bio-agent needs to infect, kill or consume those cancer cells it finds in anaerobic environments in which it thrives and human cells do not and the precise mechanism the bio-agent uses to do that will be species dependent. In phase 2, the K type drug, as a tried and tested chemotherapy drug, kills the dividing cancer cells, but thanks to the H type drugs, leaves be the normal cells which are temporarily no longer dividing. The killing of the internal flora is not required during phase 1 as indeed the bio-agent will likely have the same requirements for life as the patient's internal flora. The killing of the internal flora in phase 2 might be a medical management requirement to protect the intestinal wall from the flora while the gut wall cells are temporarily unable to divide and reinforce themselves because of the action of the type H drugs. Ringer How? Using what I have described as "type H drugs". Ringer Specifically the metabolic pathways and proteins that would be disrupted are those which usually control cellular division of cells. The type H drugs work by interfering with the control mechanisms which the body uses to stimulate or start cell division at certain times and under certain conditions and to suppress or stop cell division at other times and that interference would be designed to jam the control mechanism so as to stop cell division so long as the drug is in the body. Many types of cancer cells divide regardless of the body's control mechanisms - such cancer cell division isn't started selectively so it can't be stopped either naturally by the body's control mechanisms or artificially by pharmaceutical drugs. So I presume growth factor metabolic pathways and proteins would be suitable targets for disruption by the type H drugs. Wikipedia: Growth factor So for example, typical normal cells will wait for the appropriate growth factor to attach itself to the corresponding growth factor receptor on the cell's surface before initiating cell division. Many types of cancer have cancer cells which will divide regardless of whether there is the appropriate growth factor attached to the cancer cell's corresponding growth factor receptor or not. One obvious approach the drug developer could take would be to design a type H drug which mimics the growth factor receptor's shape and thus will selectively bind to the corresponding growth factor. If there is a lot more of the type H drug in the extra cellular fluid than there are cell growth factor receptors then the growth factor would be mopped up and leave none free in the extra cellular fluid to be available to bind to the cells' growth factor receptors, thus preventing normal cell growth from being initiated. The person is not killed as I have explained to Arete because the cessation of normal cell division is temporary and the patient's health managed and once the H type drug has cleared from the body the usual control mechanisms for cell division can resume their normal operation.
-
Arete Apology accepted. Possibly I would not have been misunderstood if I had stuck to using the term "hypoxic" for the environment and "anaerobic" for the bio-agent selected to function in tumour cores with an inadequate oxygen supply for human cell aerobic respiration. I don't see any flaw in the idea that a suitably selected anaerobic micro-organism would thrive, flourish and grow at the expense of all human cells in anaerobic parts of the body. Are you suggesting that the flaw is in the therapeutic merit of encouraging an anaerobic infection where before there was none? The therapeutic merit is that the body already has successful defences against anaerobic infections but none against the cancerous tumours this phase 1 of treatment would be infecting. In addition, medicinal drugs are available to control anaerobic infections. So the merit is in replacing a foe we can't defeat (dormant or quiescent cancer cells inside tumour cores) with a foe we can defeat (anaerobic bacteria). Arete I referred to a quote from Wikipedia - Experimental Cancer Treatments - Bacterial Treatments which yes mentioned "Clostridium novyi". Yes I can read your Wikipedia reference but do you realize that your own Wikipedia reference distinguishes between the natural Clostridium novyi which causes gangrene and the bio-engineered NT strain which is less toxic which has been researched as a cancer treatment? Arete - And routinely reside in the body, for example as gut flora, harmlessly and not causing any infectious disease. I think you would find your own quoted Wikipedia article most relevant Wikipedia - Clostridium novyi-NT - Potential Therapeutic Uses in Cancers Arete Because the fallacy of a bacterium which can identify and attack cancer cells irrespective of the oxygen saturation of the environment in which cancer cells find themselves is not simplifying the problem but rather is making the problem a whole lot more complicated. Arete - Well then one of your points was a point I had already pointed out in my OP and so was redundant to this discussion. Arete - No, phase 1 of the treatment will be effective at achieving phase 1 treatment goals, namely to eradicate from anaerobic tumour cores all viable cancer cells, whilst leaving cancer cells in aerobic periphery or rims of tumours unaffected. Phase 1 does what it sets out to do, no more and no less. Arete - I'm not in the least confused and if you need me to make it even more crystal clear to you then I will do my best to explain. My entire proposal is not flawed. The flaw is in your misunderstanding. Arete Those are medically manageable dangers, which could be managed using known drugs which can reduce the production of stomach acid and other known drugs which can sterliize the gut flora. We won't need anaerobic bacteria for phase 2 treatment. One can live quite happily without a fully functioning digestive system for 48 hours or longer if needs be. Arete - Now you are being silly. Blood cells circulate for about 100 to 120 days. Arete - Macrophages live for 6 to 16 days. That's long enough to kill rapidly dividing cancer cells. There are options if a longer phase 2 treatment is required. For example, isolating the patient in a sterile environment is one option to avoid infection for longer than 16 days. Another option for slower growing cancers would be implement phase 2 treatment in bursts, say one week of treatment followed by one week of no treatment to allow the immune etc systems to recover then alternating treatment weeks with recovery weeks until the cancer was eradicated. Arete - No, the cessation of all cell division in the body is tolerable for short periods if it is managed appropriately. Clearly there are dangers in shutting down cell division but I mentioned those in my OP. When, in phase 1 while moderating the bio-agent, or phase 2, to defend the intestinal wall while its cells are unable to divide? Either way, a patient doesn't die from short periods without internal flora - nor from longer periods if the vitamins the flora make for the body are supplemented artificially. It's not beyond medical science to keep a sample of patient flora alive in-vitro and use it to repopulate the patient's gut flora after treatment, is it? Well I live under the jackboot of UK rule so I know very well how innocent civilians can be tortured, arrested and jailed on the whim of the kingdom's officers whilst all the time the population is brainwashed to believe that this is some kind of "democracy". Anyway, this is for another topic, or another more political forum perhaps. I just wanted to put my politics on the record for posterity. It wasn't an attempt to pick Sweden out as a worse kingdom than any other kingdom. No offence meant to the people of Sweden who have my sympathies and best wishes for a republican future if they can obtain one. John Cuthber - Well it is indeed possible to wish for more than the bus service realistically will provide but let's not get too deeply into that now. John Cuthber - What we don't all know is what your point of confusion is and the point of me explaining what everyone ought to know as an answer to your poorly specified questions may eventually prompt you to explain whatever it is you misunderstand. John Cuthber - Well my approach and method wants a suitable anaerobic bio-agent and I have suggested a selection of the best anaerobic bacterium looks good for that, without ruling out other anaerobic organisms entirely. John Cuthber - Oh I see, you mean a fictitious bacterium which turns its nose up at any other food source which is not a cancer cell? I've not imagined such a beast though I think Arete suggested that finding such a beast would be "simpler" if I understand Arete correctly. No, no, the anaerobic bio-agent just consumes everything it can in the hypoxic core of tumours where it can thrive and not much anywhere else where it can't. It just so happens that what food source for the bio-agent which is to be found inside the hypoxic cores of tumours is dead and dormant cancer cells, is all. John Cuthber - No what you've said, is that anything John Cuthber can't put a proper name to must be magic. By your faulty reasoning your own birth must have been magic since you were not named until you had been born. Tell you what, let's assume that major pharmaceutical companies have the internet and the staff are allowed at work to browse this forum, shall we?
-
Type K drugs are well known as traditional chemotherapy drugs. http://en.wikipedia.org/wiki/Chemotherapy I am not naming one of those in particular because I don't have a preference for one of those well known drugs over the others. Type H drugs may not be available at all right now, I don't know, and on reflection, it doesn't have to be one single drug to perform the entire "Halt cell division!" role. If a number of such type H drugs were necessary, perhaps one drug for each of the many signalling pathways the body uses to stimulate cell division, but given in combination as one "type H drug" dose that could work too. , Now, even though I can't name any of the specific type H drugs right now - maybe no-one can - it is still meaningful to define the role of type H drugs. Yes you are entitled to question if the intended role is a realistically achievable goal, would any drug ever be able to do what type H drugs are defined as capable of doing? I say "yes" it is a realistic expectation and if you don't believe me then maybe a professional pharmacologist will convince you? Possibly you don't know enough about the way drugs work in general to get a feel for what it is realistic to expect new drugs to be able to do, hence your sarcasm, but it is misplaced and although amusing, those who know pharmacology will be laughing at you, not me.
-
When waiting at the bus stop, I can wish that my bus would turn up soon. That's wishful thinking too. Wishful doesn't necessarily mean unrealistic. Wrong. I can conceive in principle of a drug which becomes toxic only in an anaerobic environment but such a drug would only kill cells in that anaerobic environment. So such a drug would be good against anaerobic cores of tumours, as would the anaerobe bio-agent, but equally unable to distinguish between normal body cells and cancer cells in an aerobic environment. You'd still need another stage to the treatment to tackle the cancer cells in the aerobic environment. Although I can conceive of the principle of an anaerobically cytotoxic drug, I am not familiar with any examples of such whereas anaerobic micro-organisms are well known in life sciences. There is no "if" about it. Anaerobic organisms do exist and anaerobic respiration is an excellent evolutionary choice for anaerobic environments. As it happens anaerobic bacteria evolved before aerobic bacteria because there was not a lot of free oxygen in the early atmosphere. Your basic aerobic bacteria didn't evolve until bacteria which could do photosynthesis started pumping lots of free oxygen into the atmosphere and aerobic respiration became a viable evolutionary "choice" for aerobic bacteria and animal life which also depend on aerobic respiration to get going. Over 99% of the bacteria in the gut are anaerobes. Now, not all will be natural bio-agents, performing a useful biological function for the host animal, but some will be. Just because an anaerobic microorganism is not currently functioning as a natural bio-agent, but on occasion as a disease-causing organism, that doesn't mean it can't be conscripted to operate as an artificial bio-agent. So the candidate species of anaerobes are out there. The subtlety will be in picking the most appropriate organism and strain of said organism to function as the best artificial bio-agent for this medical treatment. I was more explaining than glossing but maybe you need me to explain it again? In phase one, all cells situated in anaerobic environments can be attacked and devoured by the bio-agent. It so happens that it is specifically cancer cells which happen to find themselves inside an anaerobic core of a tumour. As with house buying there are three factors which specifically identify cancer cells in anaerobic environments - location, location and location. In phase two, all cells which are dividing are killed by the chemotherapy. It so happens that in phase 2, the only cells which are dividing are cancer cells because all normal body cells have working cell division control mechanisms which the Type H drug has temporarily usurped during phase 2 treatment to switch normal cell division off. Think of phase 2 like a general who wants to put down a rebellion of misbehaving soldiers. What he does is to order all his soldiers to form ranks and then he shoots all those who don't form ranks. The Type H drug orders all cells to stop dividing. Non cancerous cells obey the order. Cancerous cells do not obey, keep dividing and then the Type K drug kills the dividing cancerous cells. I never mentioned "the Warburg effect" in my OP. Strictly or obligate anaerobic bio-agents would attack all cells in an anaerobic environment only because that's the only environment in which they have energy to do anything. In devouring cells in such anaerobic environment the specificity of anaerobe against devoured cell has nothing directly to do with how, if at all, the cancer cell is respiring. Indeed, a dead cancer cell which is not respiring at all could equally well become food for an anaerobic bio-agent. If you ask me to comment on the Warburg effect I would quote this from Wikipedia, Warburg Effect. You are barking up entirely the wrong tree. The bio-agent attacks anything it finds in an anaerobic environment. Some cancer cells just happen to be in the wrong place at the wrong time and get munched. Wrong again. Sigh. There are plenty of cancerous cells in oxygenated environments suitable for aerobic respiration. Such cancer cells are immune from the bio-agent and must be tackled in phase 2 treatment. Cell replication is critical to multi-cellular organisms in the longer term. However short periods of no cell division ought to be tolerable. No the method in phase 2 is to employ what I have named as "Type H drugs" which only act using the mechanisms for controlling cell division which are intact in normal cells but are faulty and unresponsive in cancer cells. So cancer cells don't stop dividing when they receive the Type H drug's artificial signals which mimic natural signals to stop dividing. That's the key characteristic of cancer cells - they don't stop dividing when the body tells them to stop dividing. They keep dividing and that's when they step out of line and can get clobbered by the K type drug. In your opinion. Hopefully that is true. Certainly this quote from Wikipedia looks in accord with the approach in my OP. This quote does not provide detail equivalent to my OP's description of the chemotherapy approach I would recommend for the phase 2 treatment. My OP did give credit to those from whom I have learned so much. I believe you are being unfair to compare my approach and method to "magic". I have explained how my approach kills cancer cells and not normal body cells, in both phase 1 and 2. What I have written is meaningful though perhaps not to you. No. I simply can't trust those royalist not to award me something when I am dead and can't say "No thanks". I really need to have my republican principles on the record now. From that article, this quote is misleading. Actually the low oxygen cores of solid tumours do not directly promote tumour growth and metastatic spread as the quote might imply. The direct effect of low oxygen is to make it more difficult for the tumour cells in areas of low oxygen to get enough oxygen to divide anything like as quickly and efficiently as the peripheral areas of solid tumors which have access to high oxygen levels. The way those areas of low oxygen promote tumour growth is indirectly because such low oxygen areas of tumour are highly resistant to many anti-cancer therapies, such as chemotherapy which directly target the characteristic rapidly dividing cancer cells but are ineffective against non-growing, non-dividing cancer cells in low oxygen areas. So the low oxygen areas whilst not growing particularly are not being killed off by conventional anti-cancer therapies either and it is those persistent lumps of cancer cells which provide reservoirs of cancer cells when killed peripheral cancer cells peel off like the layers of an onion to reveal a new growing layer which now gets oxygen and can grow and flake off to metastasize new tumours elsewhere. So I'd be suspicious of a hyperbaric oxygen treatment on its own. Hyperbaric might theoretically work to a degree to saturate solid tumours with oxygen, if the patient could stay in the tank long enough to promote solid tumour cores to start growing rapidly all the way through and quickly before they grow too much then immediately hit the growing cores with a conventional chemotherapy. However, that sounds like a very risky and cumbersome method which I am not recommending.
-
Suggesting a scientific approach and method for the medical treatment of tumorous cancer. Summary A scientific approach and method for the medical treatment and cure for tumorous cancer disease is suggested and described. The desired performance characteristics of suitable types of biological agents and pharmaceutical drugs and an appropriate method of employing those agents and drugs for the treatment and cure of cancer is described. Caution Neither the selection of specific agents and drugs, nor the determination of the optimal treatment regimes are described herein because the details for how best to implement the author's general approach and method to cure cancer still require further research by the scientific and medical community which it is hoped this scientific paper will inform and inspire. So the reader should be cautioned that the author does not herein publish detailed suggestions for oncologists to prescribe for their cancer patients which pills to pop when. The author is a scientist who is trying to find a cure for everyone one day, not a doctor who can cure someone today. Invitation to informed discussion This is claimed to be a realistic scientific paper, not a snake-oil-style cure-all claim. This may not be obvious to everyone because I am an amateur independent scientist, neither employed as a scientist, nor published in traditional scientific journals. I have published widely on the internet on mostly non-scientific topics and I am accustomed to debating my ideas on-line and so Im quite comfortable inviting replies perhaps as helpful comments and criticisms from fellow scientists and I can also take questions from any cancer specialists, doctors or other informed parties who take an educated interest in such matters. Approach and method One type of biological agent and 3 types of drugs are utilised in 2 distinct treatment phases, perhaps with an intermission between phase 1 and phase 2 of the treatment to review that the goals of phase 1 treatment have been reached before moving on to phase 2. Treatment Phase 1 It is proposed that phase 1 use a mild anaerobic biological agent (with the suggestion that this is mostly likely to be a selection of a mild, treatable, non-drug-resistant anaerobic bacteria, sourced from a well-characterised laboratory specimen) with which the cancer patient is purposefully infected and 1 type of drug, matched to be a known effective treatment capable in high doses of eliminating the selected bio-agent from the body or in small doses to moderate the intensity of the infection. During phase 1 treatment, after purposeful infection with the known mild anaerobic bio-agent, the anti-bio-agent drug is administered but only sufficiently to moderate and limit the intensity and systemic effects of the intended mild infection on the patient yet not overly administered to the point that the bio-agent is destroyed in-vivo before it has it has completed the designed treatment objectives of phase 1 treatment. In phase 1 of treatment, the expectation would be that the patients own immune response will be fighting the bio-agent and so the course of the infection must be monitored and bio-agent and drug doses continuously adjusted to maintain a mild infection. The objectives of phase 1 treatment The bio-agent is selected with intention that the infection should establish itself in any anaerobic cores of cancer tumours and be supervised there while the infection attacks and in due course kills those cancerous body cells in any and all anaerobic tumour cores in the patients body. The mild anaerobic bio-agent is selected and managed in-vivo so that it cannot be active, only dormant, in most of the aerobic environments of the body which are routinely supplied with oxygen via the blood, and so an appropriate selection and controlled bio-agent should not harm typical body cells so long as the infection is constrained to be mild with limited systemic effects on the body. The selected bio-agent is not intended to harm those cancer cells which are growing and dividing in an aerobic environment whether in peripheral parts of all tumours or in aerobic tumour cores which are have grown their own blood supply vessels. The dangers of a failed phase 1 treatment Too much bio-agent Inappropriate selection of a drug-resistant bio-agent, neglecting to moderate the intensity of the infection with sufficient drugs or a patients weak immune system failing to eliminate the infection at the conclusion of phase 1 of treatment could lead to a run-away infection causing serious and life-threatening infection or death. Too little bio-agent Administering insufficient bio-agent, over-use of drugs or a particularly active immune system could lead to the bio-agent failing to establish itself in all anaerobic tumour cores and a failed attempted phase 1 treatment leaving viable anaerobic tumour cores which would inevitably wreck the hopes for a successful outcome to any attempted phase 2 treatment. Treatment phase 2 It is proposed that two types of pharmaceutical drug are employed in phase 2 treatment and let's call them type H drugs ("H" for Halt cell division! ) and Type K drugs ("K" for Kill diving cells). Type H drugs - Halt cell division! At this time, the author does not know if type H drugs are ever used in medicine or indeed are even yet known to medical or biological science. However, this author does not want to wait for that research to be done but rather feels that a Eureka moment must be seized and acted upon and the time to publish is now. Administered on their own, type H drugs are apparently useless medically and apparently harmful so such type H drugs may not have been developed and produced for medical purposes and so may never be available to use medically until someone explains what such drugs could be used for. One of the main points of this paper is to make the case for producing type H drugs so that if they are not now available, the pharmaceutical industry can get busy making them available! What is described here is what H-type drugs are supposed to be able to do. Type H-drugs utilise and are intended temporarily to saturate the normal cell-signalling pathways which instruct normal cells not to divide. Normal cells with the exception of cancer cells pay heed to such cell to cell signals and it is the defining characteristic of a cancer cell that it ignores such signals not to divide and keeps on dividing regardless. The purpose of administering a H-type drug is to temporarily overload the normal signals and order an artificial system-wide cessation of all normal cell division in the body. Accordingly, normal cells which frequently divide - skin cells, intestinal wall cells, immune response cells, bone marrow cells, reproductive organ cells etc are tricked into stopping dividing temporarily, so long as the H-type drug is administered. Type-H drugs operate in a pharmaceutically reversible way and when the H-type drug clears from the body then the normal body cells which have dutifully followed the artificial signals and temporarily ceased dividing then go back to their normal operation without any permanent damage to the cell. Clearly, the administration of type-H drugs weakens the body systematically which depends on routine cell division and for so long as type H remains in-vivo then harm to the body's health will accumulate. Type-H drugs don't do the body any good on their own. Not only that, but for the purpose of treating cancer, type-H drugs do nothing directly to cancer cells either which are oblivious to the cell signalling pathways which type-H drugs are designed to stimulate. Type K drugs - Kill dividing cells In order to understand the utility of type-H drugs one has to consider their medical use in conjunction with Type K ( Kill dividing cells ) drugs. Type K drugs are known to medical science. They have been used to try to treat cancer but the problem with them is that they tend to kill all dividing cells, not just cancer cells. OK, well the smarter reader will see by now where we are going with Type H drugs. After administration of a Type H drug which suspends normal cell division but does not affect cancer cell division, the administration of the Type K drug is now a no-brainer. The dividing cancer cells get killed by the Type K drug. The normally dividing cells don't get killed by the Type K drug because they are no longer dividing thanks to the administration of the Type H drug. After the dividing cancer cells have died all that remains to be done is to clear the Type K drug from the body while the Type H drug is still in operation. Then later it is safe to discontinue the Type H drug at which point the body will resume normal cell division, free from cancer. The dangers of a failed phase 2 treatment The patient will be rendered vulnerable to infectious disease because of the predictable effect of the Type H drug which will prevent parts of the immune system from responding to infections. Worse case of course is that an opportunist infection may kill the patient. If the Type H drug is not as effective as intended, if the dose is too low, if it is too quickly cleared from the body then the Type K drug will kill normally dividing body cells as well which cripple multiple body functions which depend on dividing cells and worst case kill the patient. Without a successful phase 1 treatment which has previously killed anaerobic tumour cores, phase 2 treatment will only kill cancer cells dividing in aerobic environments leaving any and all remaining viable anaerobic tumour cores to provide an inexhaustible supply of cancer cells into the aerobic parts of the body. Phase 2 on its own cannot cure cancer; only after a successful phase 1 can it do that. Conclusion The Type H drugs are the biggest uncertainly in the author's mind but if they can be sourced and can work as described then conceptually this looks like an excellent scientific approach and method for the cure of tumorous cancers. Credits Thank you to all those from whom I have learned so much. Dedication This cure for cancer paper is dedicated to my mother who lives still and to the memory of all my friends and relatives who have died from cancer for whom this cure is too little and too late. This cure for cancer paper is also dedicated to Condoleezza Rice who has inspired me to understand that I may not be able to control my circumstances as a scientist without employment as such but I can control how I react to my circumstances. Condi's mother also died from cancer and she has participated in Race for the Cure events. Prizes. I do not want the Nobel Prize for Medicine or indeed any Nobel prize so long as Sweden remains governed as a kingdom. I want nothing from the Swedish King nor from any King nor Queen. I am a republican and only wish to receive prizes, awards or recognition while living or posthumously from republics or at least from non royal institutions which find themselves in the unfortunate circumstance of operating as I do inside a country currently governed as a kingdom.
-
Afghanistan: Obama's counsel of despair. Drawdown or ROUT? Could a feeling of strategic despair pervading the White House mean President Obama's drawdown plan could turn into an unseemly rout of US and other NATO-ISAF forces? It looks to me like President Obama is getting some "Dark Counsel" as regards pulling out from Afghanistan. First to explain the phrase "Dark Counsel". Have you seen Lord of the Rings? Remember King Theoden and his adviser, Grima Wormtongue, who told him he was weak, could not fight and hope to win, turned out Grima was secretly an agent for Saruman? OK remember now? That's "dark counsel". So who is giving Obama, "dark counsel", who is his Grima Wormtongue? Well maybe a lady called Robin Raphel, a former agent for Pakistan, a Washington Lobbyist in the pay of the Pakisan state. Obama has taken her on into her team, in charge of non-military aid to Pakistan, that's billions of dollars worth. Raphel is the enemy within. I would not let this woman within a mile of the White House, but there again, I'm not King Theoden, I mean, President Obama. Now instead of a "counsel of despair", I offer a simple explanation of "what went wrong". First let's compare and contrast the Afghan war to kick the Taliban out of Afghanistan (12 years, 3000+ coalition deaths and seeking a peace with the enemy who is still threatening a come-back after we pull out next year)withthe Gulf War in 1991 to kick Saddam's Iraqi forces out of Kuwait (5 weeks bombing campaign, a 100 hour ground campaign. 500- coalition deaths - a decisive coalition victory)So wars can be won, quite easily if your generals go about it the right way. The issue is that we have not declared and prosecuted a war against the imperial power in this case, Pakistan. Have a more detailed look at how our generals confronted the imperial power, Iraq, in that Gulf War. Quotes from Wikipedia: Gulf War First there was the 5 weeks bombing campaign - then the 100 hour ground campaign Smokin' Now, imagine if instead of that excellent Gulf War battle plan, we had decided to invade Kuwait by air drop and then asked Saddam if it was OK to supply our air-dropped troops in Kuwait by supplying along Iraqi roads and we would pay him billions of dollars to let us? How would the Gulf War have gone then? Saddam would have had us by the balls then like Pakistan has us by the balls now. You can't defeat the troops of an imperial power by asking that imperial power for permission to do it. You have to defeat the imperial power. The front line troops, whether Saddam's forces in Kuwait or Pakistan's Taliban forces in Afghanistan are only the tip of the enemy war machine. You have to hit the enemy in the rear, hard. And we've never given Pakistan the kind of air war that we gave Saddam in 1991. So Pakistan is laughing at our war campaign in Afghanistan. Now do you understand how easy this war would be to win? We have to confront and defeat the imperial power, Pakistan, whose auxiliary, irregular or paramilitary forces the Taliban are. Well if you still don't know how to win, no worries because I do, so just put me in charge of this war if you want it won.
-
The requirement to defend military supply lines in war, to expect the enemy to attack and to attempt to cut any long supply lines is a basic part of classical military strategy. If there was ever to be a sustained resistance to our invasions of Iraq and Afghanistan then any competent military strategist could have predicted that the enemy would wish to attack our supply lines in Iraq and Afghanistan and if we didn't do the correct thing according to classical military strategy and defend those supply lines then it was inevitable that the enemy would mine and ambush our undefended, or poorly defended, supply lines. Now the US does indeed have academic military experts who do indeed know the importance of this requirement in war and have published relevant articles on the internet, such as this fine example - Army Logistician Supply Line Warfare by Dr. Cliff Welborn but that ancient yet essential military knowledge, that ought to be taught to every officer at every military academy, doesn't seem to be in the brains of the US, British or other NATO generals, who seem to think "patrolling" or "ever bigger MRAPs" is a better plan to try to keep our soldiers safe on otherwise undefended supply routes. Actually, the better plan is simply establishing a secure perimeter around your supply route which is watched 24/7 from static guard posts all along the route, either side of the route, and a mobile reaction force to reinforce wherever and whenever the enemy concentrates to attack the supply route. I've suggested in this thread a detailed plan to defend supply routes in Afghanistan but no doubt there are many variations on that theme. Don't get me wrong, big MRAPs have their uses as a back-up if and when the enemy makes it through the defended perimeter of a supply line but there does clearly need to be a secure perimeter established in the first place otherwise your supply routes remain effectively uncleared territory and anything on the route not protected by tons of armour is simply easy meat for the enemy. Certain items in my plan, about seizing satellites and what to bomb in Pakistan is new, specific intelligence for the war on terror and is maybe a bit much to expect on day one from our military. But for military leaders not to know the requirement to defend supply routes, and therefore foolishly to lead our soldiers to die from enemy road side bombs and ambushes - this is unforgivable ignorance on the part of our generals, defense secretaries and Pentagon, NATO and UK MOD civilian support military "experts". Those in charge don't seem to know the military basics. It's like the donkey-generals who led brave lion-soldiers to their deaths advancing on foot against machine gun nests as in world war 1 - all over again. It's another famous military disaster and it is no way to win a war (even though we will likely win this war on terror eventually but at a very high cost in blood and treasure.)