Luc Turpin
Senior Members
-
Joined
-
Last visited
Everything posted by Luc Turpin
-
 Finaly, I have been res Good one!😊 Will try and give you more than that!
Finaly, I have been res Good one!😊 Will try and give you more than that! -
Ok, well then we don't understand much about it. True, we don't understand the fundamental of why it works; speculation is part of science too; trying to pull new evidence into the picture and then see where it goes. Trusted evidence is most of the time in the eye of the beholder; or what is in line with your beliefs is good evidence and what is not in line with your beliefs is not good evidence. I will continue posting my friend and see if something intrigue's you in believing that it might not be as we think it is.
-
This is what I think! If most of the evidence is taken into consideration on mind and brain then these statements are mostly correct. “The perspective of the role of the body as a sensory array for engaging life experiences that basically support the metabolic/homeostatic imperative of the brain and brain function.” “Through homeostasis, mind emerges as an efferent response to afferent stimuli. Even more, mind is evinced by and is exclusive to behavioral expressions that suggest a thought process. “ “What could possibly be more to the foundation of mind than the engine and energy that powers the brain functions generating the mind. Mind, to be clear, doesn't exist without brain function and brain function does not occur without the energy driving that function.” “Relative to the body, the science informs me that the body is merely a vehicle that facilitates the brain's survival imperative.” If all of the evidence is taken into consideration on mind and brain (including old-ignored and newer) than these same statements need to be revisited or statements added to those. We do not know what consciousness is, let alone how it works. We do not know how the brain really thinks beyond synapses and chemicals. Also, the body does more than we think it does and nature thinks more than we think it does. That is what I think! I have presented arguments, information and evidence to that effect in past posts and will continue to do so in future ones. correction: We do not know how the brain really thinks beyond synapses and molecules.
-
Notwithstanding, the results point toward memory being preserved in the body. I understand what you are implying; only the study authors could answer your question. I doubt that going through the “rough-terrain” would be sufficient to grow tougher skin, but it remains a possibility. Did not understand the link that you wish to make between waves generated in the brain and the “domino effect”! I beg to differ. As I have already stated, the brain has the principal role while body actively participates in memory, emotion, cognition. For emotions and the gut microbiota, that relationship is more tightly linked than anticipated. “The brain can impact the gut and the gut can impact the brain”. Its influence is also much more considerable than anticipated. The brain may very well create the emotion, but the microbiota regulates it. “The gut microbiota can modulate anxiety-and depressive-like behaviors”. “Gut microbiota regulates mouse behaviors through glucocorticoid receptor pathway genes in the hippocampus”. “….the microbiota is necessary for normal stress responsivity, anxiety-like behaviors, sociability and cognition”. Also, the “microbiota maintains central nervous system homeostasis by regulating immune function and blood brain barrier integrity”. It also “influences neurotransmitter, synaptic, and neurotrophic signalling systems and neurogenesis". I reiterate, the gut microbiota plays a prominent role in emotion. So much so that at times one wonder’s whom is doing what to whom. And that is the microbiota alone; imagine then what role the whole body plays on memory, emotion and cognition. It's the author's perogative to say that cells have the "capacity to think". As for the immune system, I would say that it is at least a very complex system in of it's itself and is very good at what it does. As for virus, you would be surprised at what they can do!
-
I will be slower this weekend at responding as this is a weekend of festivities for family and friends
-
Just kidding; lyrics not evidence; It was too easy to pass! Is it random molecules masquerading as "thinking"? Authors give the impression that is does not seem so! https://scitechdaily.com/breaking-the-brain-muscle-barrier-scientists-discover-hidden-neural-network-like-abilities-of-self-assembling-molecules/ This should have been a stand alone post, not attached to Dim post!
-
Missed this one! For memory, I offer the flatworm experiment and organ transplant references. For emotion, I offer the microbiome and two way conversation via the vagus nerve. "We know that in animals the gut microbiome can affect emotional behaviour via the vagus nerve." https://www.universiteitleiden.nl/en/news/2022/05/stimulating-the-gut-brain-nerve-can-influence-emotion "This narrative review summarizes key aspects of vagus nerve function as a main player in the microbiota-gut-brain axis in depression" https://www.sciencedirect.com/science/article/pii/S2666915323001464 3.For cognition, speculation with a touch of research on cells and thinking. "Do cells think" "A microorganism has to adapt to changing environmental conditions in order to survive. Cells could follow one of two basic strategies to address such environmental fluctuations. On the one hand, cells could anticipate a fluctuating environment by spontaneously generating a phenotypically diverse population of cells, with each subpopulation exhibiting different capacities to flourish in the different conditions. Alternatively, cells could sense changes in the surrounding conditions - such as temperature, nutritional availability or the presence of other individuals - and modify their behavior to provide an appropriate response to that information. As we describe, examples of both strategies abound among different microorganisms. Moreover, successful application of either strategy requires a level of memory and information processing that has not been normally associated with single cells, suggesting that such organisms do in fact have the capacity to 'think'." https://pubmed.ncbi.nlm.nih.gov/17530173/
-
My mistake, he did discard the head part, but the point remains that the tail part grew a head and remembered the task, so where was memory stored before a new head was regenerated. The head part of the worm would have remembered the task, because heads store memory. Are you clicking on the links and nothing happens or are you cliking, they open and you expect highlighted text? If its the former, please click on the boxes provided below the post for access and if is the latter, I have not highlighted anything, because it is a quick read. There are clear indications that thinking and memory storage happens in the brain. However, I would venture only at this point that collective consciousness proponents would say otherwise or indicate that it is both as mind and brain form a whole. Like brain appearing to form a whole with the body, except that in the case of mind outside of brain, its a physical entity forming a whole with a non-physical one. A radio without a signal. The only observations hinting at it for me are episodes when a malfunctioning brain is able to spit out any kind of thinking when that should not be the case. Notwithstanding, I believe that there is no proof per say that this hypothesis is even worth bearing in mind. I offered it for discussion, because it is one of many being considered. Again, my position is not that we should be pursuing this or any other model, but that there is something wrong with our current picture of how mind works in the brain. I will get more info on the mind through brain hypothesis and get back to you. Din't catch that one and good one sayiing that the brain has a hard time adapting to death Wow! The Who! Like that one! And body and cells appear to adapt to circumstance to stay alive and do the business that they have to do! And remember that the pinball wizard was "in a quiet vibration land"; so maybe it is also the case for mind!
-
Correction: Mind from brain and body: Brain plays the predominant role in mind while body provides energy, stimuli and senses, but also actively participates in memory, emotion, cognition etc. They might even create their own memories, emotions, cognition which are amalgameted with those produced by the brain to form the whole.
-
My main contention in our discussion remains that evidence-observations do not match up with our current understanding of how mind works. More on this later. As for "categories' being used in the discussion, here is a simplification that may help in understanding: Mind from brain: Mind is the exclusive domain of the brain with body providing energy, stimuli and senses to the brain Mind from brain and body: Brain plays the predominant role in mind while body provides energy, stimuli and senses, but also aids in memory, emotion, cognition etc. Mind through brain: The brain and body become conduits for mind residing outside of the body and brain. The mind is the signal and the brain is the television set. I have used these categories in our discussion, because I believe that they help a bit in comprehension. But do be reminded that they are mine and arbitrary in nature. Hence my opening statement that the main topic of discussion is about data not matching up to evidence rather than mind-brain categorisation. I hope this helps a little, and indeed I believe as well that we don't agree on the nature of the partnership. I think that your position is more in line with the mind from body model, while mine is more in line with the mind from brain and body model. In light of this being a discussion broader than categorisation, here are two links to newer findings that I would like you to comment on: Brain waves found to travel in one direction when memories are made and the opposite when recalled.url Evidence early, but emerging, that gamma rhythm stimulation can treat neurological disorders.url So, are we not moving a bit the needle here in determining that it is not only about synapses and molecules, but maybe also about waves and frequencies? Or am I the one stuck in the past still thinking that the neuro-science field is even now only contemplating molecules and synapses? Note: These are but only two of many examples of studies finding out that waves and frequencies affect the brain. Or, more broadly, that the brain does not work as expected. Brain waves found to travel in one direction when memories are made and the opposite when recalled.url Evidence early, but emerging, that gamma rhythm stimulation can treat neurological disorders.url
-
Imagine that it did and that we would have to go fetch it everytime it ran away! My-my, me being silly again 😊 https://www.scientificamerican.com/article/brains-are-not-required-when-it-comes-to-thinking-and-solving-problems-simple-cells-can-do-it/ Scientists researching the field believe that there is memory transfer. It could probably be the same kind as in the flatworm memory transfer experiment. Yes, I know abut DNA
-
Note: The use of the term “let’s be honest” in my previous post was intended to the few who are reading this thread and greeting my every word with possible contempt. I do not believe that you are doing so. You are just not in agreement with me. A mind through brain model is not required to explain memories from organ transplants nor physical transformations due to multiple personality disorders. What is required is a modification of the mind from brain only model to a mind from brain and body model. However, what would constitute an indication of mind through brain is your suggestion that a head trauma patient coming out of a coma would begin speaking a foreign language unknown to him before the trauma. I do not believe this to be possible, but would nonetheless constitute probable evidence of mind being processed through the brain, if it was so. Citations were not provided as a diversionary tactic, but as demonstration that something may be wrong with our current understanding of mind. Some of the evidence provided is anecdotal while some is not. Conversely, studying this subject matter is not easy to do so. It is also not on the radar scopes of most institutions financing research. To that effect, the burden of proof does not lie with only one, or a few, but the entirety of it all. It is highly doubtful that all of it is wrong. This also goes for other citations given throughout this thread as well as in the preceding “mind” thread. What is at issue here is that citations and argumentation do not entirely concur with a “perspective of the role of the body as a sensory array for engaging life experiences that basically support the metabolic/homeostatic imperative of the brain and brain function.” This is the topic that we should be debating at this point in time, not if mind through brain can even be possible. Digressing here, but how so?
-
First, there is nothing in my last post to you that tends towards showing mind residing outside of brains; only that the body may play a more prominent role in mind than anticipated. Second, let's be honest here; based on the strict definition and application of the mind from brain only model, who would seriously have expected that an organ transplant would lead to memory transfer and major personality changes? Or that a multiple personality disorder would bring about such dramatic physical transformations! I am sure that some of you were surprised, even perplexed by this. At the very least, this needs to be acknowledged. Acknowledgement is also warranted for other material posted by me that were both unexpected findings and inconclusive of mind from brain. How can the possibility that organs have and pass on memories or other findings previously provided in this thread fit in tightly and neatly with a mind from brain only model? Do remember that memory to cells was also the conclusion in the flatworm experiments provided earlier. And that electrical fields affect body shapes! This also unexpected. I am not making any point here; the observations are! Without forgotten-new observations, there would be no need for contemplating other venues for mind. Congenital blindness does not entail mind loss, but brain transformation, as would be expected from either a mind from brain or mind through brain model. If one considers for a moment both possibilities that cells hold memory and that memory is held in a holographic state as suggested by Paul Peitsch and his dissection experiment, then a missed hand would diminish, but not eliminate memories. So, the change would be so subtle as for it to pass unnoticed. Even, major body parts being absent would not diminish substantively as the principal actor in all of this remains the brain. As for mind itself, some of what is indicated above for memory might apply, but it is probably dictated more by the principle that a small amount of simple cells brings about a simple mind while a large amount of complex cells brings about a complex mind. Do be reminded that humans are amalgamations of cells and that the delineation between brain and the rest of the body is ours in the making. Finaly for this, the notion of simple and complex minds, if such is the case, would apply jointly to mind from brain and mind through brain. As for sunshine and rain, they are not part of the physical system of brain having a depression. In this circumstance, they would then not count as valid examples for discussion. "Psychological effects are not evidence that pieces of the mind reside elsewhere", but, conversely, it does not preclude it either. Notwithstanding, memories in the body and major personality changes following organ transplant might hint at it while physical transformation from a mental disorder suggests a much tighter coupling than anticipated of mind, brain and body. The magic resides in the brain, but a magician’s hat is needed at the very least to pull a rabbit out of it. I am not a lone wolf owling at the moon. As show from studies posted, others have joined the chorus. You are speculating that they had to go at it many times before learning and that they grew thick skin. Again, possible, but highly doubtful. The part of the head was conserved, grew a tail and remembered the task. You are also speculating about heads sections remembering faster than tail sections. In the study, there is no mention of either thick skin or faster recall. If they controlled for this, I do not know. Please read my last response to DrmDoc In of itself, this is a very bold statement that you are making about cells remembering. It would change a lot about the mind brain conncection, and biology.
-
Analysing data without being too anxious about it, generally leads to a different understanding of the situation. I know this, because when I am anxious, I almost always get it wrong. My take on it is that there is some, but not major concern. We need human data; we need also other kinds of data points and analyse all of this within context.
-
Get your point, but that is not what the researchers doing the study concluded. Why would "thicker skin" suddenly appear. possible, but quite unlikely. First, mind through brain is one hypothesis, not necessarily mine. Mind needs brain to think and do every day stuff. What mind looks like without a brain is not really known as it is always being processed by the brain. However, some say that when the brain is quieted, through meditation, drugs or NDE's, something happens that might be an inkling of mind without brain looks like. Highly-highly contentious though. And yes, some drugs do quiet the mind. Brain, being a physical entity, needs a break sometimes and goes to sleep, leaving mind in the lurch. Well, if the references that I provided in one of my posts are even half correct, we might have to entertain the notion of upgrading the bodie's effect on brain and mind.
-
Having difficulty posting! Many of your posts on this thread have been very informative, balanced and representative of science. Context is needed to interprete data. I also agree with INow that anxiety may be leading the way in reading and interpreting the data.
-
Maybe our mind from brain theory should be renamed the mind from body theory!
-
You are right! Then, I concede! On this matter only!😊
-
I admit that I cannot be sure without doubt that its the same memory as the original. But, I persist in saying that this memory appears to be less maleable to time than others. Cold reality of an artifical heart I line with what was just posted on organ transpants, but in a patient with an artifical heart. https://www.seattletimes.com/seattle-news/health/cold-reality-of-an-artificial-heart/ Should have been posted separately Sorry Dim.
-
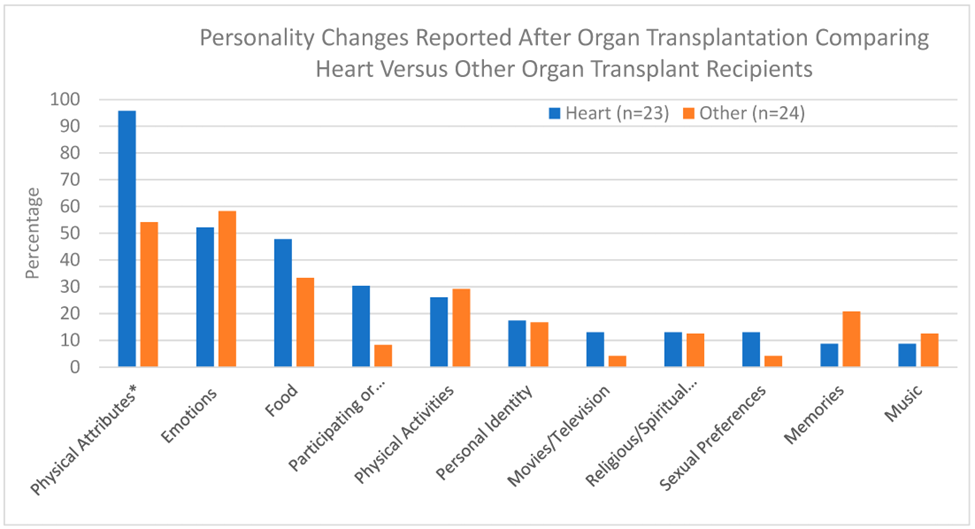
Amputation causes a whole cascade of effects: depression, anxiety, self-esteem issues, distorted body image, change in personality, cognition impairment, change in body schema. Most are probably actuated by the brain, but how would we know if it was not, in some small sense, also coming from the body? How could we disentangle the two? __________________________________________________________________________________________________________ Where it gets interesting is for organ transplants, “Personality changes may occur following organ transplants: In some case, organ recipients report personality changes that parallel the personality of their donor; Some organ recipients “remember” events from their donor’s life. Cellular memories stored outside the brain may transfer information from organ donors to recipients." https://www.psychologytoday.com/ca/blog/the-leading-edge/202402/do-organ-transplants-cause-personality-change-in-recipients#:~:text=In%20some%20cases%2C%20organ%20recipients,from%20organ%20donors%20to%20recipients. “When excluding changes in physical attributes, 89.3% of all transplant recipients reported experiencing a personality change after receiving their organ transplant.” https://www.mdpi.com/2673-3943/5/1/2#:~:text=Among%20heart%20transplant%20recipients%20who,four%20or%20more%20personality%20changes Another article presenting types of personality changes Physical Attributes* 19 (95.7) 13 (54.2) 32 (68.1) Temperament 14 (60.9) 12 (50.0) 26 (55.3) Emotions (happy, sad, etc.) 12 (52.2) 14 (58.3) 26 (55.3) Food 11 (47.8) 8 (33.3) 19 (40.4) Participating or Watching Sports 7 (30.4) 2 (8.3) 9 (19.1 Physical Activities 6 (26.1) 7 (29.2) 13 (27.7) Personal Identity 4 (17.4) 4 (16.7) 8 (17.0) Movies/TV 3 (13.0) 1 (4.2) 4 (8.5) Religious/spiritual Beliefs 3 (13.0) 3 (12.5) 6 (12.8) Sexual Preferences 3 (13.0) 1 (4.2) 4 (8.5) Memories 2 (8.7) 5 (20.8) 7 (14.9) Music 2 (8.7) 3 (12.5) 5 (10.6) Art 0 (0) 1 (4.2) 1 (2.1) Colors 0 (0) 0 (0) 0 (0) Electronic Devices 0 (0) 2 (8.3) 2 (4.2) Political views 0 (0) 1 (4.2) 1 (2.1 ANY (excluding Physical Attributes) 21 (91.3) 21 (87.5) 42 (89.3 file:///C:/Users/Dad/Downloads/preprints202309.1894.v1%202.pdf “Changes in heart transplant recipients that parallel the personalities of their donors” http://individual.utoronto.ca/mfkolarcik/HeartorBrain2_Pearsall-Journal%20of%20Near-Death%20Studies_2002-20-191-206.pdf A theory about it! "Can an Organ Transplant Change A Recipient's Personality? Cell Memory Theory Affirms "Yes"" https://www.medicaldaily.com/can-organ-transplant-change-recipients-personality-cell-memory-theory-affirms-yes-247498 _________________________________________________________________________________________________________ And it gets really interesting is in dissociative identity disorder where the brain actually changes the body. "The different identities, referred to as alters, may exhibit differences in speech, manerism, attitudes, thoughts and gender orientation. The alter may even present physical differences, such as allergies, right-or-left handedness or the need for eyeglass prescriptions. These differences between alters are often quite striking". https://namimi.org/mental-illness/dissociative-disorder/didfactsheet#:~:text=The%20different%20identities%2C%20referred%20to,the%20need%20for%20eyeglass%20prescriptions. "These include the abrupt appearance and disappearance of rashes, welts, scars and other tissue wounds; switches in handwriting and handedness;" . https://www.nytimes.com/1988/06/28/science/probing-the-enigma-of-multiple-personality.html “Multiple personality disorder has been associated with marked psychophysiologic alterations ever since careful clinical observations have been made on this perplexing disorder. Physical symptoms known to be associated with multiple personality include headaches, conversion symptoms, changes in voice, seizure-like activity, unexplained pain or insensitivity to pain, alterations in handedness or handwriting style, palpitations, alterations in respiration, gastrointestinal disturbances including bulimia and anorexia, menstrual irregularities, sexual dysfunction, and dermatological conditions including unusual allergic responses and differential responses to medication. Early scientific studies on the galvanic skin response in multiple personality disorder were conducted by Prince in the erly twentieth century. Since 1970 there has been a resurgence of interest in multiple personality disorder including sophisticated studies of physical symptoms, brain-wave activity, visual evoked potential, regional cerebral blood fWw, visual refraction, muscle activity, cardiac and respiratory activity, galvanic skin response, and the switch process. In addition to describing these studies, the etiology of multiple personality disorder and future directions in research will be discussed.” https://core.ac.uk/download/pdf/36679938.pdf “Visual function in multiple personality disorder” “Background: Multiple personality disorder (MPD) is characterized by the existence of two or more personality states that recurrently exchange control over the behavior of the individual. Numerous reports indicate physiological differences, including significant differences in ocular and visual function, across alter personality states in MPD.” “Results: Physiologic differences across alter personality states in MPD include differences in dominant handedness, response to the same medication, allergic sensitivities, autonomic and endocrine function, EEG, VEP, and regional cerebral blood flow. Differences in visual function include variability in visual acuity, refraction, oculomotor status, visual field, color vision, corneal curvature, pupil size, and intraocular pressure in the various personality states of MPD subjects as compared to single personality controls.” https://pubmed.ncbi.nlm.nih.gov/8888853/#:~:text=Results%3A%20Physiologic%20differences%20across%20alter,and%20regional%20cerebral%20blood%20flow. “Individuals with dissociative identity disorder (DID) have been known to show varied skills and talents as they change from one dissociative state to another. For example, case reports have described people who have changed their handedness or have spoken foreign languages during their dissociative states.” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2766827/#:~:text=Individuals%20with%20dissociative%20identity%20disorder,languages%20during%20their%20dissociative%20states. If this evidence-observations are correct, how does this fit in a mind from brain model? But, It may be a magician's hat with many surprises in it!☺️ The memory did not decide, but just did become indelible. This memory feels different than other, but I cannot prove without a shadow of a doubt that it cannot be maleable through time. However, everytime I tell the "story", it does not change.
-
Apologies, woke up more susceptible for no apparent reason yesterday. Your participation in this thread is essential. Your knowledge, your intelligence and your sound theory on mind-brain pushes me to think and rethink things as we progress in our discussion. I believe that one of our main differences between you and I is about certainty in the matter of mind and brain. You believe, based on knowledge-observation acquired a while ago (no disrespect intended here) that mind is created by brain. While I believe that more recent evidence-observation indicates that it might not work like that, that it might be mind through brain. I reiterate that the "jury" is still very much out on this one. What makes it difficult for both of us in this discussion is that there would be only subtle differences between both in how the brain would appear to operate. So most of the evidence-observations that supports the mind from brain would support either one, while newer findings appear to show at least that it might not be that simple, that something is amiss, that it might be a different type of operating system. Take for example the topic of interplay between brain and body. You see it as the brain taking what resources it needs from the body and creating mind on itself. While a mind through brain theory could (as in not a definite possibility; given for example only) see mind being expressed in the brain and body and expressed differently in the brain than in the body. The consolidation of the appearance of mind, whether coming solely from brain or from a "montage" created by brain and body, would be very similar in appearance and be hard to differentiate from one another. One has body in a supporting role while the other has body in a participative role, but both have similar outputs (mind). Brain takes in what it needs from the body and makes it happen, while mind goes through brain and body with different outcomes which are collated together to create mind (not entirely sure of this last statement, because it brings up the binding issue). No disagreement as to the foundation of mind, but the picture does not end at the foundation. There is apparently a lot that sits on top of the foundation. Mind needs brain and body to fully express itself in a mind through brain theory. Energy is required for both theories to work. Yes, evidence and observations have been incredibly clear, but this evidence-observations does not rule out something else at play. We are both right on mind from brain, but I might be wrong on even entertaining a mind through brain scenario. I too, most of the time, enjoy our exchanges. The onus is on me to make them always pleasurable. They have sharpened my perspective also. You know much more than all of us who have participated so far in this thread. By the way, Chalmers was saying that we do not know of brain creates mind, not the opposite. No consensus not because there isn't sufficient evidence, but because of different interpretations of evidence.
-
Could be that it changed or was not what actually happened, but this memory has an indelible character to You very well know that I was not talking only about the enteric system, but the possible interplay between brain and body as a whole. Mind is a holistic process with brain doing the heavy-duty work and body possibly doing some of it. Its an interplay, not a one-way. It's a painting, where most of the painting is done by the brain and the body fills in the gaps to create the whole. I gave references to that; not coming from me, but from others. Mind-brain interaction is much more than homeostasis and energy balance and metabolism. I have said that you are right in all of your assertions, but evidence-observation tend towards a picture that is more than this. Not that you are wrong, but that there is more. You always come back with a categorical position with no movement and no consideration for evidence-observation. No consideration, only rebuttals. I am always wrong in all of my statements, even when backed with possible evidence-observations. All positions are categorically rejected without even slight consideration. Then, why do we even bother discussing if I am always wrong and there is not even the slightest chance of movement? If "I do not grasp the nature of thought and mind in its most basic form", then others more versed on the matter than I do so and have said that the story is incomplete. By the way, Chalmers won his bet and there is still no consensus in neuroscience on how the brain creates the mind. That is not me talking, but the whole of this science field. You say you know, without an inkling of a doubt, which is not possible in science. One theory supersedes another when data becomes available, or at least the theory is tweaked to take into consideration new information. No tweaking possible here. Ceci n'est pas une discussion mais une conversation de sourd.
-
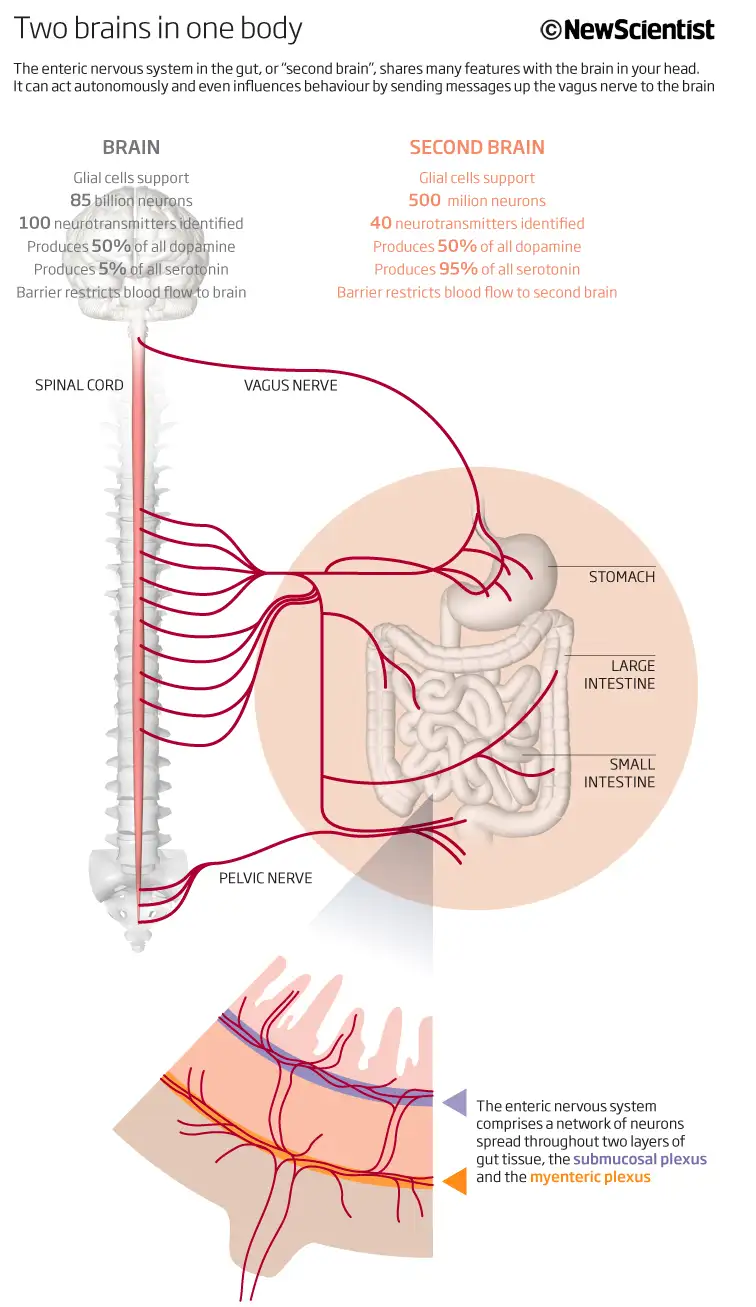
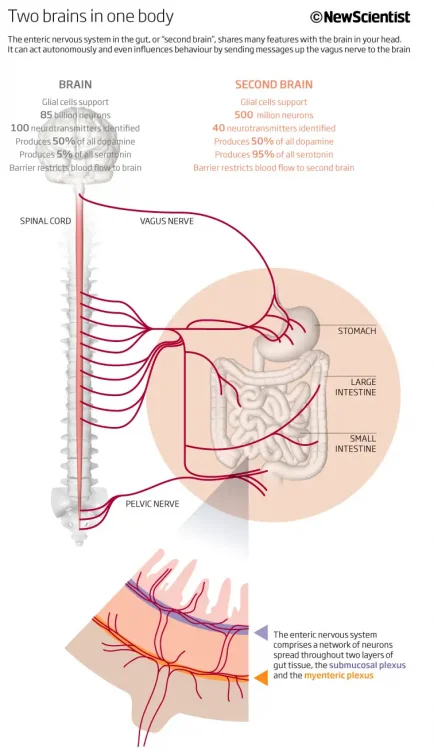
Only fueling the generator or also participating in the dance? getting harder to tell! The enteric system can work separately from the nervous system. "The gut-brain axis is a bidirectional communication network that links the enteric and central nervous systems. This network is not only anatomical, but it extends to include endocrine, humoral, metabolic, and immune routes of communication as well. The autonomic nervous system, hypothalamic-pituitary-adrenal (HPA) axis, and nerves within the gastrointestinal tract, all link the gut and the brain, allowing the brain to influence intestinal activities, including activity of functional immune effector cells; and the gut to influence mood, cognition, and mental health." https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6469458/ "How gut bacteria are controlling your brain" "Over the last few decades, researchers have started to uncover curious, compelling – and sometimes controversial – evidence to suggest that the gut microbiota doesn't just help to keep our brains in prime working order by helping to free up nutrients for it from our food, but may also help to shape our very thoughts and behaviour. " https://www.bbc.com/future/article/20230120-how-gut-bacteria-are-controlling-your-brain "Thinking from the gut" "The gut-brain axis seems to be bidirectional—the brain acts on gastrointestinal and immune functions that help to shape the gut's microbial makeup, and gut microbes make neuroactive compounds, including neurotransmitters and metabolites that also act on the brain." https://www.nature.com/articles/518S13a#:~:text=The gut-brain axis seems,also act on the brain. Gut instincts: The secrets of your second brain https://www.newscientist.com/article/mg21628951-900-gut-instincts-the-secrets-of-your-second-brain/ I could dig deeper into the data to find how complex, integrated and interchangeable the roles appear, but evidence and observations tend to get lost in the discussion. This is one of many attemps to resolve the easy problems. All of them do not address the hard problem. If it did, Chalmers would have lost his bet in 2023. Bold-large text not mine. "The easy problems are easy precisely because they concern the explanation of cognitive abilities and functions. To explain a cognitive function, we need only specify a mechanism that can perform the function. The methods of cognitive science are well-suited for this sort of explanation, and so are well-suited to the easy problems of consciousness. By contrast, the hard problem is hard precisely because it is not a problem about the performance of functions. The problem persists even when the performance of all the relevant functions is explained … What makes the hard problem hard and almost unique is that it goes beyond problems about the performance of functions. To see this, note that even when we have explained the performance of all the cognitive and behavioral functions in the vicinity of experience … there may still remain a further unanswered question: Why is the performance of these functions accompanied by experience? A simple explanation of the functions leaves this question open … Why doesn't all this information-processing go on “in the dark,” free of any inner feel?"
-
You need to be near death to have an NDE; some have them without being near death, but they are rare and no one knows the mechanism to activate it. It would be unethical to bring someone near death to study it. For the rest, I am not sure what you mean. Because you brain is offline and it is needed to be conscious. Your mind transforms the signal, which becomes your own mind. If you are not looking at the show, then you are not making memories to store. No one knows why near death, unconscious or anesthetised, someone would suddenly wake up, be aware and have memories. It is the same for "mindsight" experiences; how can someone blind, even from birth, be able to "see" in some fashion or another his surroundings and experience it? It you think while asleep it is because you are not entirely asleep. The body apparently participates with the brain in thinking and memory storage. The piece with the head and the piece without the head grew respectively tails and heads and all remembered the skill. Meaning that that memory skill was stored in the body of the part without the head while it grew one.
-
Not saying that time actually slowed-down; when I am bored, time seems to pass slowly and when I am not, it seems to pass faster; all a matter of perception. So, guess I was really bored during my experience, as it felt as if time had almost stopped 😊 "felt as if soft-gentle hands took control of my handle bar and turned it to the right"; who said it was a ghost? still just an impression of, not something that actually occurred; why would I be saved by a ghost and not others who get into an accident and die; I am not special. The story has remained exactly the same for all these years, without tweaks to suit the mood; I am aware that memories are rewritten and noticed that some of my own change in tone and texture over time, but not this one. It is engraved in my memory. Yep, software needs hardware to run, but the software is more complicated to understand and have it work as it does than the hardware.