

CharonY
Moderators
-
Joined
-
Last visited
Everything posted by CharonY
-
I think taking over would not be trivial. It is not like China has a foot in the door and while economic ties have deepened, there was always an anti-mainland sentiment first from the older generation, because of remembered history, but the Taiwan eventually became democratic and younger folks now are for the most part not willing to give it up. So a soft takeover seems very unlikely, but how would a military takeover look like? A full on invasion is more likely to trigger a defensive response, and especially Japan will push for it. If China gets away with a military takeover, many other countries will become very nervous indeed. Otoh I wouldbe surprised if the Chinese government does not realize that such an action could further destabililize the situation and am not sure whether they think it would be worth the risk. I would think that they will try their hardest to get pro-China support and use that to make a semi-soft power projection.
-
I do not think your assessment is accurate (except in the vaguest possible sense). Taiwan's history is complex with many changing hands. But if we start in the late 19th century to the end of WWII, Taiwan was a Japanese model colony and a blueprint of what the Japanese vision of a Pan-Asian system under Japanese rule might have been. Toward the end of WWII there was also a civil war in mainland China between Chiang Kai-shek, leader of the Republic of China and Mao Tse-tung. Chiang eventually lost and fled to Taiwan, which he declared to be new seat of power of the Republic of China. For some time they were seen as the legitimate government of mainland China in exile, though obviously that did not hold for very long. So technically if there was a mutiny, it was committed by the People's Republic of China against the Republic of China (and not the other way round).
-
The characterization is a bit strange as agricultural exports are barely a blip in Taiwan's economy, its largest exports have been electronics for a long while. The trade volume with the US is not huge, but still totaled 100 billion which is about 70-80 billion less compared to Germany or UK. This would still roughly place Taiwan among the top 10 US trading partners. I would also argue that especially due to its location Taiwan would be a strategic asset.
-
I am not aware of web-based tools. Most that I have used require some time of database of retention times for time correction and many are integrated into certain packages (such as Skyline). There are also others, including commercial packages, but I never used any of them Ultimately I found it easier to just create your own database using reference standards as the predictions were not super accurate and I found them most useful except to screen out compounds (might be different for you application). But especially with modified peptides things are tricky. I faintly recall an open source model that was called OPERA-RT (I think). But have no experience with it.
-
I actually wanted to write a topic on that paper but more in form of a critique, then forgot about it. Luckily here is an article that echoes a lot of my thoughts on it. https://arstechnica.com/science/2021/11/mobile-clusters-of-cells-can-help-assemble-a-mini-version-of-themselves/
-
1) they are not necessary, but depending on t quality of your sample prep it can help reduce contamination, and improve signal quality however, 2) depending on the volume of your zip tips (10 vs 100 ul, for example) and the sensitivity of your instrument as well as you should have enough to see something. But if whether you see enough depends on your sample and application. Generally I see significant loss of protein digests (up to 70%) and that may or may not be an issue for you. You often also lose e.g. very hydrophilic or very hydrophobic peptides along the way. If you have a very well defined and/or low complexity sample, I would use them, especially in conjunction with a nano-LC to keep your system happy. If purity is an issue, I would also use them. However, if sample loss is the dominant issue, then it may not be the best way. 3) I would not do it. Theoretically you could try to regenerate the material, but you will like get cross-contamination and the capacity might degrade. 4) can't think of any papers off the top of my head. Most that describe their use have some weird modifications which presumably help with sample prep, but in real applications rarely had any impact (in my experience).
-
That is certainly true. Most students do not realize that a lecture is supposed to be a general guidance to the material, and is not the material itself.
-
I would also add that effectiveness is typically more dependent on the student than on the lecture itself. Lectures generally gives you an idea of a topic with some examples. However mastery of the subject requires additional engagement with the subject. At least if you want to go beyond just the next exam.
-
Related to that here is an interesting article that highlights that rebuttals might be effective in combating science deniers. https://www.nature.com/articles/d41586-021-02152-y Actual performance varies by audience, I am sure. Though we had good experience with folks who actually came individually to information sessions. Whereas if a bunch of connected folks appeared, they seemed to reinforce their beliefs. One thing that is also somewhat concerning is that quite a few folks were citing youtube videos as source. That makes it (by design, I would say) more difficult for folks to figure out where these folks get their "info" from.
-
Actually, the logic goes the other way around. If everyone is vaccinated, then it would effectively mean that the virus has already a reduced virulence and kills fewer people. As such there is less pressure to reduce virulence than in an entirely unvaccinated population where hosts are killed at a higher rate. However, one should take those arguments with some caution- these are only general trends. What actually happens in a population is obviously more complex and depending a combination of factors the there might be local optima for a certain combination of virulence and infectiousness. Or to put it differently, it is difficult to predict which trajectory a given virus is going to take at any given time. What we can say is that with a higher reservoir of folks carrying and producing the virus, we have a higher chance of continuously seeing new variants.
-
I would also like to posit that this may already be the case within the human population. Younger folks tend to have milder or no symptoms, while being able to transmit the disease (and young adults tend to be also on the more mobile side). One should therefore be careful to assume that lower virulence is inevitable or that it may happen on a quick timeline. There are also some other features (e.g. transmissibility prior to symptom development, as well as asymptomatic transmission) that could make it stay lethal for quite a while.
-
No, generally not. Competition against delta is a bit of a benchmark as it is currently the dominant variant in most areas. Something able to inch it out is a matter of concern. The only favourable outcome I can think of is if omicron turns out to be causing only mild symptoms. In that case you would want it to replace delta.
-
Going back to omicron, retrospective analyses indicate that omicron has been around in Europe as early as Nov 18 (i.e. before their identification): https://www.bbc.com/news/world-europe-59473131 While its potential to cause severe illness compared to delta is not known yet, the fact that it seems to be spreading (even in the background of delta) is of concern and worldwide efforts have increased to monitor their presence, both in retrospective (as the one linked above) or prospective surveillance. While the data could be biased due to ongoing efforts, preliminary data suggest that in SA omicron might be outcompeting delta. I have attached a figure showing the frequency of mutations in alpha, delta, and omicron in three of the genes (darker colour indicates higher frequency of a given mutation). Considering seemingly high transmissibility already indicates that the additional mutations in alpha do not hamper its effectiveness in infection. The important bit to figure out now are the health risks and then how well vaccinations are holding up.

-
That is very much expected. Preventing infection also prevents death from illness. Your original question was asking for evidence of efficacy of preventing infections, which you have received (repeatedly). And just to prevent a few rounds of arguing semantics I would like to point out some common usages in epi-data: "Infection" commonly refers to all positive tests, regarding of symptom status. Technically it refers specifically to the virus, but for communication with the broader population (e.g. via dashboards) it is sometimes conflated with COVID-19 infection (or similar). While this is technically inaccurate, it is simply a messaging strategy as the population was found to be more familiar with the name for the disease than for the virus. "Asymptomatic" is used if a positive test is found, but the patient does not present symptoms at time of testing. The issue is that folks are typically not tracked over time, so in some cases folks are actually pre-symptomatic (i.e. develop symptoms later in the infection process). Often the status of the patient at testing is not documented at all, so the frequency of asymptomatic cases is usually not well established. Moreover, in several areas testing strategies have switched to testing symptomatic cases only. As such in literature you will find a large range of estimates of symptomatic vs asymptomatic cases. Vaccine efficacy is the ability of the vaccine itself to improve disease outcome. This is generally done in controlled trials and historically this is based on disease presentation (i.e. showing symptoms of the disease). One of the reason is that in many diseases individuals do not spread the disease if they do not present symptoms (often indicating a low viral load). Due to the ability of pre-and asymptomatic spread of SARS-CoV-2 transmission is also monitored, but it is not as easy as tracking of symptoms. Vaccine effectiveness is basically a measure to look how efficacy translates into reality. This is done by capturing data during vaccine rollouts in an observational study. Here, it is important to segment the cohort according to the specific question. I.e. for example look at infected vs non-infected groups and check the vaccination status. Or conversely, segment for vaccination status and check for the variable of interest (e.g. infection rate or hospitalization).
-
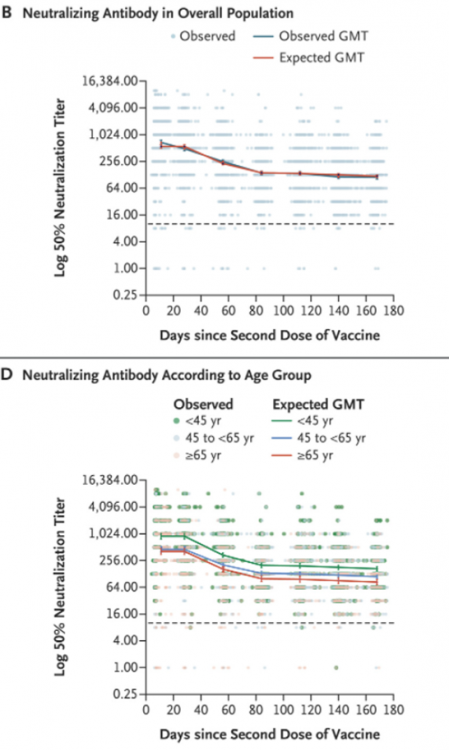
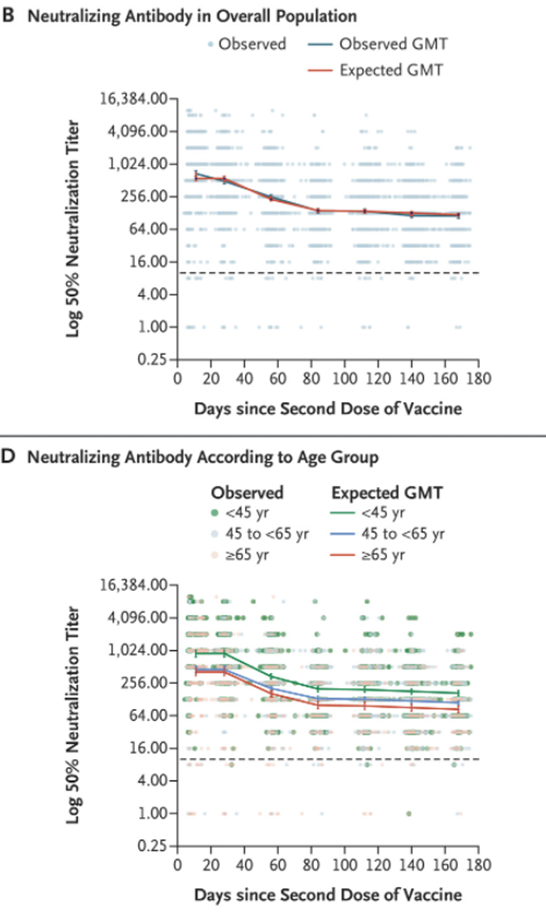
@Sensei From this study: Levin et al. DOI: 10.1056/NEJMoa2114583 I have attached two graphs showing the 50% neutralization titer after Pfizer-BioNTech vaccination as well as an age-separated graph. It shows the decline within 6 months which can correlate to some degree with lower resistance to infections, especially with fast developing infections (such as delta), though as mentioned before, it is only one piece of the puzzle. The dots are the actually measured values, showing quite a range of individual responses.
-
The data provided by Swansont as well as the REACT-1 data from the UK both indicate lower infection rates in vaccinated folks. Indeed, but if you are wondering about the impact of vaccinations, you need to know the proportion of vaccinated folks in that graph. If for example the vaccine was 100% effective in preventing infections, the data could only contain unvaccinated folks and then the differential death rate would necessarily be caused by something else (e.g. age differences).
-
I don't think that this is even actually relevant. The original hypothesis was that vaccines are only (or mostly) effective protecting against developing symptoms. The poster did not spell it out and went on a tangent with an anecdote, but I took it as assuming that it is ineffective at preventing spread. That is also the only way the overinterpretation of the supplied graph in a later post makes sense. The focus is on transmission, so that is the element that needs to be traced in vaccinated and unvaccinated folks. The critical point that needs to be answered with regard to efficacy of the vaccine to curb spread is the difference in infection rate between these groups, which the poster continues to ignore (and which already has been posted). With regard to graphs I remember a few, but most are not neat comparative analyses, mostly individual patients with either condition (e.g. infection with SARS-CoV-2, one of the vaccinations etc.). I could pick out some if you'd like. However, it is important to note that antibodies are not telling the whole story when it comes to immunization. In all cases of infection and immunization the various antibody titres decline (but with vastly varying kinetics). However, an important of the adaptive immune system is the eventual formation of memory cells. Long-term protection is mediated by these T and B cells, as opposed to circulating antibodies. In the case of a new infection, these cells are necessary to produce new neutralizing antibodies to combat that disease. This is why even vaccinated folks with low circulating antibodies can mount effective responses, when exposed to the virus. Even in cases of successful infections (which practically means that the virus is able to replicate until they go over the sensitivity limit of established tests), the virus can be cleared out without resulting in associated damages and symptoms. Thus, declining antibody titres alone are insufficient to fully establish protective levels of a vaccine over time. That being said, a faster decline could indicate overall reduced responses, which see for example in the elderly. Recent infection data does indeed suggest that in these groups antibody titers decline faster and unfortunately also become more vulnerable to infections and sever outcomes (or to put it differently, the differential outcome between vaccinated and unvaccinated started to shrink in this group).
-
Please demonstrate how the infection rate among vaccinated is the same as among the unvaccinated based on the graph. What, in fact is the proportion of vaccinated folks in that graph. In case you forgot, you made two claims in the sentence. While mechanistically that is somewhat true (prevention of serious conditions is around 80%, depending on age and time of last jab, and reduction of infection of infection is about 50%), the provided data does not allow you to draw these conclusions. The minimum parameters that need to be established are how many among the infected are vaccinated or not (i.e. is there a bias between these groups). A second thing to establish is the age of infected in the last compared to the previous wave. Another, more technical issue is also how effective the testing program was in either time period (e.g. looking at test rate and test positivity). A simple alternative explanation (which is only partially true, but you would not know without looking at additional data) is that the third wave might have been driven by unvaccinated young folks, who have a reduced risk of dying.
-
Except of course that that data tells us nothing about the impact of vaccinations as the data is not separated between vaccinated and unvaccinated folks. The study above detailed that aspect by looking at differential infection rates and indicated the said difference (i.e. vaccinated folks have a third of the infection if using crude numbers, about 50% if adjusted for age and other factors). The sample size is meaningless if the necessary details are missing and therefore do not provide any information related to your claims.
-
IIRC, the cases in that report were based on cases before delta. The latter was found to have higher breakthrough rates. Not that it changes the argument, just nitpicking the actual numbers.
Read Elliot et al. Science 2021;eabl9551. It provides a comparison between vaccinated and unvaccinated populations.
Vaccinations reduce viral production and accelerate clearance and as such do mitigate infections to some degree. While breakthroughs still occur, risk of infection is about cut by half to a third, even with the delta variant. Risk of passing it on after transmission is also reduced a bit. But as delta seems to have a low infectious dose, the risk is still substantial. But especially in conjunction with masking and other public health measures we and others see less spread after a given outbreak after introduction of vaccines. That being said you are not wrong, with the disease getting endemic, new variants are bound to appear eventually.
Yeah, fair enough. My trust in the ability of humanity to pull together has been tested heavily. And I foresee a failing grade. Just like my class.
Or alternatively we forget all lessons learned within a few years and things will again go down the drain when feces hit the spinning thing again.
Important Information
We have placed cookies on your device to help make this website better. You can adjust your cookie settings, otherwise we'll assume you're okay to continue.