CharonY
Moderators
-
Joined
-
Last visited
Everything posted by CharonY
-
I think there may a couple of wrong assumptions but I am not read enough in those areas to provide an immediate in-depth response. Let's talk about zoonotic diseases first. One thing of note is that at high population densities and contacts with animals there is a higher likelihood of a pathogen crossing species barriers. But even then they may not cause large outbreaks, as they may have low transmission or low virulence and either exist invisibly in a given population or do otherwise do not garner a lot of traction. Many viruses re-assort in pigs transfer to humans and then change further (e.g. by grabbing genes from other viruses in their hosts) before they cause outbreaks. Take the H1N1pdm09 (swine-flu) pandemic, for example. That particular strain has a bit of a mosaic structure, probably originating from three parental pig viruses and emerged into humans somewhere in North America, some assume in Mexico. There is also the MERS epidemic, that came likely from camels but were sufficiently contained not to cause an epidemic. Hantavirus is a deadly virus that has a case fatality of ca. 40%. However, it is spread by mice and not human to human (luckily) and was found in the USA. There are also plenty of zoonotic diseases found in India, such NIpah virus and has been slowly spreading. However as there is no human-human transmission the spread is not as rapid. Likewise, we had a Zika pandemic not so long ago, a mosquito borne disease, originating from Africa. Japanese encephalitis likely originated in the Indonesia-Malaysia region and while it is also transmitted by mosquitos, it causes outbreaks every couple of years with about 13-20 thousand deaths each year. Again, lucky break that they need mosquitos as vectors. So in a way to me the question is whether it is by chance that those originating from China have larger impact on global health and economy or whether there are factors contributing to it. I think one needs to think beyond sanitary issues, as you mentioned. One question could be for example how connected China is compared to India. But also for example how the meat industry looks like. Another perhaps simple question is also what types of potential zoonotic diseases are there that could for example mix with animals that come into close contact with humans. In India many are mosquito borne, but perhaps they are less relevant in China. In Europe and US industrial pig farming has a huge potential to recombine and spread viruses in pigs, but there are perhaps fewer animals around that can spread novel viruses into pigs. Regulating or closing those market can likely close some of the risk factors. However, ultimately my thinking is that the world is shrinking, for better or for worse. There will be more contact between each of us and there are diseases that not zoonotic. What it means is that otherwise local disease have a much easier to become epidemic and even pandemic. Without the willingness for rapid responses to detect human-human spread, I think that most of the measures will be insufficient. And I think it is somewhat wrong to think that in the Western world our measures will keep us safe indefinitely. We had prion disease entering the food chain (sure it is not an infectious disease per se, but still). Farm animals often have to be culled due to various disease outbreaks. So far those have not managed to jump the species barrier, but it is not something that may so forever. On the other hand of course there is the tendency of diseases to become less virulent over time (as killing the host is generally not a good long-term strategy) but in the meantime a lot of harm can be done. Other man-made reasons for outbreak are for example anti-vaccination campaigns. HIV/AIDS now is well controlled, and we get complacent again (in the 90s it was for a time the leading cause of death in young adults). We have tons of pathogens that can mix, mutate and while there may be area with larger reservoirs than others, I do think it is dangerous to think it as an "elsewhere" problem. I think this is what lead to complacency when China was facing COVID-19 and that is why despite ample warnings the Western world only reacted when they had deaths in their midst. It may not be quite what you are thinking of, but I do think that this change in mentality is necessary to combat the inevitable occurrence and re-occurrence of diseases (and I apologize for all the typo and rantiness, it is more flow of thoughts without proper editing, may try to express it clearer when I got time again). Edit: had so many unfinished thoughts but wanted to include that global warming is going to increase the likelihood of many, especially mosquito borne diseases, so that has to go in there also somewhere.
-
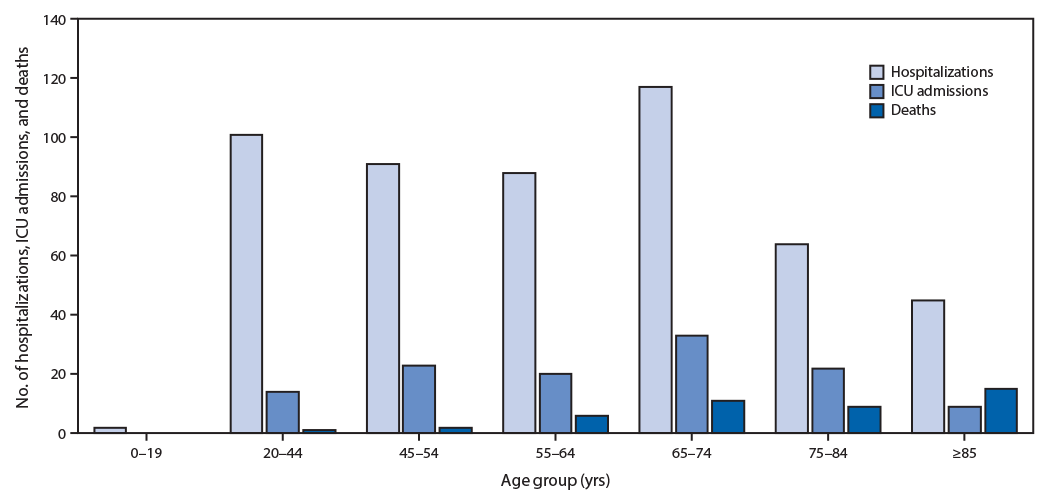
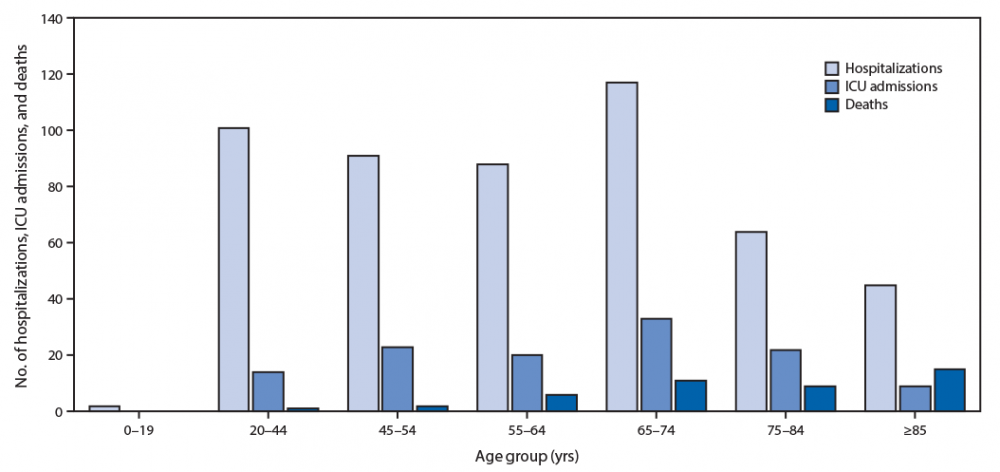
Yes, cardiovascular issues are associated with worse outcomes, for example (based on Wuhan data). But also note that all age groups can have more severe outcomes requiring hospitalization. The US is still undersampled but initial info shows almost all brackets affected except 19 and younger based on CDC data a couple of days ago:
-
Also pre-existing conditions.
-
Well, there are recommendations for decontamination of hospital bedding and clothing. Heat alone is seemingly insufficient for full decontamination based on above data, but a combination of heat/detergent/bleach might be. For sun light one might calculate the output for UVC and see whether that may be high enough, I suppose.
-
I am not sure, ozonation, UV treatment and disinfectant fogging are being used in certain biocontainment facilities, but I don't know whether they would work and/or may be harmful in patient care facilities. The latter are often more crowded than biological workspaces and patients are more vulnerable to ozone, for example. I know that fogging is not allowed but I don't think that there are recommendations regarding UV and ozone in patient care (to my knowledge). Theoretically one could establish a protocol with thorough ozonation followed by quantitative ventilation or quenching to ensure safe levels. But again, I do not know if folks have tried or studied that.
-
I vaguely remember such data but am not sure whether it was about viruses. I am going to have a look. Edit, took a quick look and while it is not the paper I had in mind, but there is one on SARS-CoV-1. UV radiation source was placed 3 cm above the sample. UVA (365nm) emitted 2133 µW/cm2, UVC(254nm) 4016 µW/cm2. Note TCID50 is a measure of viral titer (by assessing the titer at which 50% of the host cells show cytopathic effects). So it looks that in most cases a short exposure will result in incomplete inactivation, especially under less ideal conditions. Edit forgot to add: Darnell et al. 2004 J Vir Met 121:1 85-91. They also looked at temperature: at 56 C much was inactivated after 20 min, but active viral particles could still be found for at least 60 min. 60C most inactivated after 4 min, but still incomplete after 60 min. 75C authors claim full inactivation after 40 min.
-
I think it is because it is roughly the recommended time to run the UV light on bio benches. Kind of a default setting.
-
You mean the origins? That is part of a large discussion with quite a bit of unknowns. I think most think that they are a version of mobile genetic elements, like transposons or plasmid, but more autonomous. However another line of thinking, especially among folks working on giant viruses think that they might be stripped-down cells from an unrecognized domain of life. I think the latter has some traction in certain areas but is still considered the less likely narrative by most folks, I would say. Or do you mean how viruses are formed by their host cells? There are different pathways, but in all cases essentially the viral genetic load is transferred into the host cell which is then used to produce viral proteins as well as propagate its genetic material. There can be steps in between (such as reverse transcribing the RNA in case of retroviruses, for example). At some point the virus particles are packaged with the genetic material and they then escape the cells. This can e.g. happen by lysing the host cells, budding or exocytosis. The two latter processes result in enveloped viral particles.
-
The graph shows trajectories in the number of cases and it does show that in most cases they will rise further.
-
Yes, that is what you normally do as an impact statement. However, such studies have been conducted since at least the 2000s. While it does not mean that it is not worthwhile pursuing, it probably does mean that it is difficult to translate it into an effective treatment. I have not checked whether any trials have been conducted but it is not uncommon (actually far more common) that promising preliminary studies do not translate well into clinical utility.
-
Sorry genetics and evolution does not work like that and I suggest opening up a new thread if you want to discuss that further (we have hijacked quite a bit already).
-
That is not the how the terminology is usually used. The gene pool for humans has precisely the same age. There is difference in diversity or gene flow (e.g. due to isolation) but there is nothing that is older or newer per se. Increase in genetic determinants of resistance to certain disease stems from selection for that (e.g. by pathogens but also co-selection) within a given population but you can have higher susceptibility e.g. in Africans and lower elsewhere. The higher genetic variance is a different factor and only means if a selective sweep happens, there is a higher chance of finding individuals with higher fitness (but does not mean that a given individual in a given population is actually a carrier).
-
Sorry, I was not clear above. They actually also used in vivo models in the previous studies, however in all cases (including the study in the quote) the viral particles were treated with the surfactant or they were co-administered with the surfactant . I.e. it is not that the animals were treated and then infected or rescued by treatment, which would be important for practical use. Yeah, although at the beginning he made certain suggestions such as somhow protecting elderly and then let the infection sweep. Which was dismantled pretty quickly by health officials and then he backtracked. But at least he is not doubling down and thereby risking lives.
-
The limitation of that study is that the virus had to be pre-treated with the surfactant to become less virulent. In the follow-ups I also only see co-treatment or in vitro assays. It is unclear how you would employ it in an in vivo situation. If the virus is already in, there is a good change it won't do any good (or you may have pump so much into the patient that it becomes harmful). It is sad that folks forgo the health information provided by the same administration.
-
That is not true at all. In Africa different societies existed ranging from the nomadic groups you mentioned to fairly large empires. One of the best known is the Songhai empire (15th-16th century). Among the cities within that empire Timbuktu and Djenne were powerful commercial entities. There are of course far more examples (Aksum, Kingdom of Ghana, Abyssinia to name a few). What I am saying is that the view of Africans as nomadic tribes is Westernized colonialist view that is not in line with actual history and I would urge caution to build any generalizations from this level of misinformation. And before we get to that, in the New World, it is the same, indigenous people had built complex societies in nations, which, while different than their Western counterparts, were highly complex political and societal system and had various levels of urbanization that were not too different from certain Western nations of the same time. Of course the situation shifted when we come closer to the time of the Atlantic slave trade but it is erroneous assumption that all there was were nomadic (and often also assumed to be primitive) tribes.
-
There are cases reported there. South Africa is at 554 cases, Nigeria at 44 for example. There are more, but there are not enough tests in a number of countries.
-
What part do you object to? The only one I can think of is that the persons in question (other than Columbus of course) were born in the 19th century and lived to the 20th. But every person I was familiar with in that group had formal academic education and in the cases of the engineer, additional training on top. I am therefore not sure what the point. Medical professionals have academic training followed by residencies. How is that different? Clearly I am not understanding your point here. Back to OP, self medication is not a good idea, apparently.
-
Well balance should still be factual. I do not know De Havilland but Parsons received engineering training at an engineering firm after his studies in mathematics. I do not want to derail it further but if one needs to dig back two centuries and still not find plenty of examples it does somehow indicate the rarity of such achievements, no? Meanwhile there are countless unnamed, non-famous with training labouring away to provide all the basic information we have on this and other diseases (at times, at personal risk) which are summarily dismissed because obviously what they do is too mundane and boring. Instead, we long for stories of the untrained underdog saving humanity by having flashes of genius that are misunderstood by those actually working on it. It sure is a great Hollywood story but it sure ain't what's happening.
-
Basically because there is not enough data to make any meaningful inferences. There is a bigger chance that some more resistant alleles will be found in Africa, but so far no dice. I have no idea what a "new" race is.
-
She was studying at a time where it was generally prohibited for women and ultimately produced a dissertation. She also taught at university in her 20s. I.e. her whole career was rather academic (not to mention private life, being the daughter of a mathematician).
-
What you need are antigenic elements, you cannot easily isolate them from people. Or rather it is far easier to propagate it, and then create an inactivated form rather than injecting humans samples which are hopefully inactive (but may also carry other nasty stuff). So much of it is surface removal, too. However, considering that cell are constantly pumping out virus particles, also into the bloodstream and there are mechanisms for cell-to-cell transmission, I doubt that any physical removal would really provide a net benefit. A lavage is mostly used for sampling (at least afaik, we use to obtain lung fluid samples not sure whether there are other medical reasons.).
-
Indeed, typo on my part, my apologies.
-
Many other countries in Europe have similar trajectories as Italy or at least China. The optimistic scenario (China delays and in the meantime other countries implement measures and draft plans to slow down or even stop outbreak) clearly has not happened. Responses were conducted after the horses were out of the barn (I.e. rising deaths, which again are a bad indicator unless in retrospective).
-
I am repeating myself, but I find it extremely confusing (and disappointing) that folks see what is happening elsewhere (good and bad) and somehow decide that it does not apply to them or that there are no lessons to learn. Italy's (and before that Wuhan's) health system is on the brink of collapsing and apparently there are no lessons to be learned from that. Meanwhile there were successful measures elsewhere in use for the last few months and now it is being discussed whether one should consider them in the first place. In world where information transfer is so fast, this seems almost medieval. I have got grad students who are rightly worried and then at the same time undergrads who think the "free time" now is the right opportunity to party. Sometimes I feel that folks only got two modes, ignoring the situation and utter panic. There is apparently no setting for measured response. Edit: again I should say that in Asia a number of countries actually opted for early measured responses (though to be really fair one should add that there were also panic peaks), which makes the current state even more ridiculous.
-
From what I have read most think that the situation in Japan is still unclear, there is comparable little testing done considering the timeline (one of the few countries testing way below capacity). The latest data indicates that about 20k folks have been tested so far, of which 1k have been found positive. On a different note, rates of detection and deaths are somewhat informative when it comes to active situations (i.e. the slope of the respective curves) and it does seem like in Germany the death rates are slowly catching up. Most cases are still active, unfortunately. Without measures to curb spread, there is a risk of that the situation in Italy (overwhelmed medical system) will be repeated through the rest of Europe.